Prabhat Barnwal, Yuling Yao, Yiqian Wang, Nishat Akter Juy, Shabib Raihan, Mohammad Ashraful Haque, and Alexander van Geen ask,
Is the low COVID-19–related mortality reported in Bangladesh for 2020 associated with massive undercounting?
Here’s what they did:
This repeated survey study is based on an in-person census followed by 2 rounds of telephone calls. Data were collected from a sample of 135 villages within a densely populated 350-km2 rural area of Bangladesh. Household data were obtained first in person and subsequently over the telephone. For the analysis, mortality data were stratified by month, age, sex, and household education. Mortality rates were modeled by bayesian multilevel regression, and the strata were aggregated to the population by poststratification. Data analysis was performed from February to April 2021. . . .
Mortality rates were compared for 2019 and 2020, both without adjustment and after adjustment for nonresponse and differences in demographic variables between surveys. Income and food availability reported for January, May, and November 2020 were also compared.
And here’s what they found:
All-cause mortality in the surveyed are was lower in 2020 compared with 2019, but measures to control the COVID-19 pandemic were associated with a reduction in rural income and food availability. These findings suggest that government restrictions designed to curb the spread of COVID-19 may have been effective in 2020 but needed to be accompanied by expanded welfare support.
More specifically:
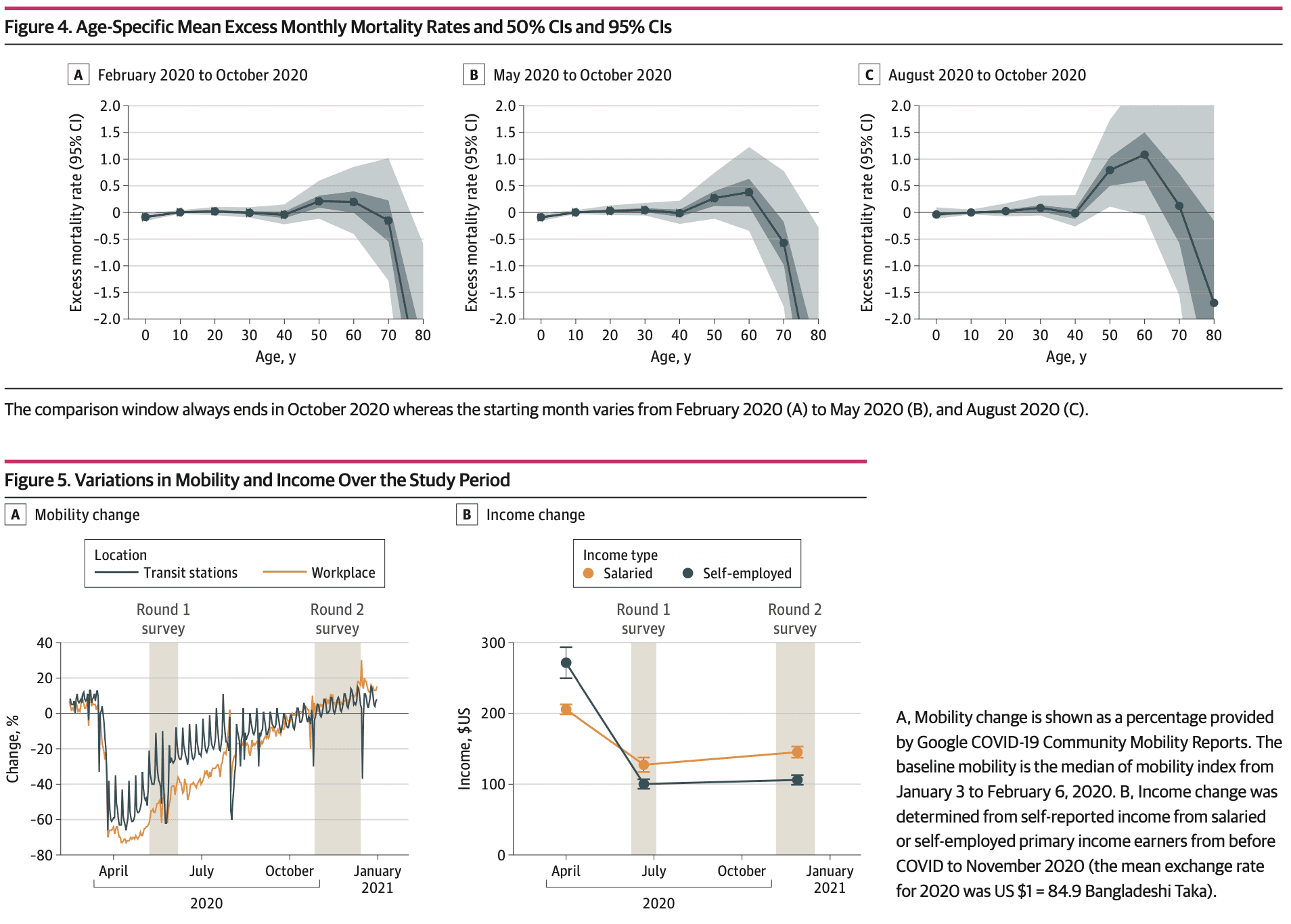
Enumerators collected data from an initial 16 054 households in January 2020 . . . for a total of 58 806 individuals . . . A total of 276 deaths were reported between February and the end of October 2020 for the subset of the population that could be contacted twice over the telephone, slightly below the 289 deaths reported for the same population over the same period in 2019. After adjustment for survey nonresponse and poststratification, 2020 mortality changed by −8% (95% CI, −21% to 7%) compared with an annualized mortality of 6.1 deaths per 1000 individuals in 2019. However, in May 2020, salaried primary income earners reported a 40% decrease in monthly income (from 17 485 to 10 835 Bangladeshi Taka), and self-employed earners reported a 60% decrease in monthly income (23 083 to 8521 Bangladeshi Taka), with only a small recovery observed by November 2020.
I’ve worked with Lex and Yuling for a long time, and they both know what they’re doing.
Beyond the direct relevance of this work, the above-linked article is a great example of applied statistical analysis with multilevel regression and poststratification using Stan.
deb –
> To me, the interesting fact about the data reported is that Bangladesh seemed to have super strong immune, respiratory, nervous, digestive systems after millenia of unnatural selection…
Given that as I recall you’ve posted other comments about “the immune system,” I wonder if you have strong priors that you bring to your thinking about cause/effect there. What evidence do you bring to apply your generalized beliefs to this specific context?
For example, you say:
> “To me, the interesting fact about the data reported is that Bangladesh seemed to have super strong What is interesting is what gave them group protection in spite of food insecurity and other uber-stressors. At the very least, this supports the keep your immune system tuned up idea.”
What information do you have to infer that
“Bangladesh” (as some undifferentiated mass of people) have relatively “super strong immune, respiratory, nervous, digestive systems after millenia of unnatural selection” (and what do you mean by “unnatural selection”)? What evidence do you provide that your analysis of comparative “Bangladesh” immunity is anything other than conclusion driven?
Deb –
> …It is surprising Bangladesh did not show the same pattern as similar natures.
I get that part of your argument. I’m trying to figure out what the test of your argument is. What is your evidence that “Bangladesh” has a more robust immunity system than non-“Bangladesh,” let alone “super strong” immunity (along with other “super strong” systems)?
I’m guessing that you have no empirical evidence re the “Bangladesh” immune system? Reverse-engineering from what you find surprisingly low excess mortality numbers is what I’m asking you about. There might be an infinite number of reasons the excess mortality might be lower than you’d expect. A “super strong” immunity system strikes me as an unlikely explanation given the average baseline nutritional status in Bangladesh.
I’d guess something along these lines:
https://www.tbsnews.net/coronavirus-chronicle/covid-19-bangladesh/ventilators-enough-no-63079
Probably also oxygen shortages, inability to enforce NPIs in the villages, and so on.
A quick Google search yields New Zealand, Taiwan and Norway all experienced a drop in mortality rate between 2019 and 2020.
Interesting, essentially countries that didn’t have strict NPIs in place for one reason or another. It seems that could be a fruitful starting point for explaining what happened.
Anyone who published on this correlation would be nitpicked to death though, while the same people wouldn’t bother for papers concluding whatever they already agreed with. So wealth/power weighted collective opinion wins.
I don’t know how we get to actual science from here. I guess we need a medical Tycho Brahe to go out and actually collect reliable health data.
This would then allow testing quantitative models. Also, the type of data collected should be driven by the various models, so there is a positive feedback loop here once it gets going. Medical research is like an engine waiting for that spark of ignition.
Wait, you’re saying New Zealand didn’t have strict NPIs in place? WTF man? New Zealand had some of the strictest controls on the planet! “From a global perspective, New Zealand stands out regarding the efficacy of its approach to combatting the spread of COVID-19, having effectively eliminated the virus from its territory. Towards this end, the country resorted to a draconian lockdown of its borders and its domestic economy. Following a month during which the country shut down all nonessential businesses, restricted internal travel, and banned social gatherings, New Zealand was able to rapidly reopen its economy.” That’s from this Brookings Institute report https://www.brookings.edu/articles/policy-and-institutional-responses-to-covid-19-new-zealand/#:~:text=Throughout%20the%20pandemic%2C%20New%20Zealand,virus%20and%20prevent%20further%20outbreaks.
Phil. the huge advantage New Zealand had was that it controlled its borders extremely well because it’s an island nation. After shutting off all travel into and out of the country (as I understand it), it was able to do a relatively short strongly enforced lockdown, conclude that basically there was no virus in the country after that, and reopen. So the duration of the strict restrictions internally was less, due to the lack of cross border travel.
I understand that a couple outbreaks are thought to have started by frozen foods harboring virus? But basically there was a very low risk in the country because no travel across borders and small population that complied fairly strictly with the quarantine.
If Anon’s thesis is that the stress of the lockdown and the loss of incomes and etc etc were in part responsible (I personally don’t agree with that model) it is consistent to say that NZ had less of that stress due to shorter duration of intense lockdown.
My understanding is that NZ (and Taiwan) are island nations that effectively closed their borders and so it didn’t have much internal effect in 2020. Ie, people weren’t being put on ventilators, etc because they tested positive or prevented from visiting with their elderly relatives for most of that year.
From your link it sounds like they had like 1 month of “lockdown”. Otherwise it was normal:
https://www.theguardian.com/commentisfree/2021/dec/18/from-covid-free-to-delta-and-back-new-zealands-year-of-living-almost-normally
Of course, it was called racist in the US to close the borders early on. But it probably wouldn’t have been very effective anyway.
Yep Daniel. The idea is that positive covid tests lead to both both actual covid and various inept medical and public health interventions.
Eg, Cameron Kyle-Sidell saved more lives in the US than anything public health authorities did, and got removed from the ICU in March 2020 due to it:
https://vimeo.com/402537849
But other frontline doctors agreed and stopped that inept intervention once they heard his account. And where did the ventilator idea come from? Anonymous rumors from China that got added to treatment protocols based on literally no evidence. That was from the “evidence-based medicine” group who reject all sorts of cheap and safe (but possibly ineffective) interventions until some study is done. Only expensive and dangerous interventions can be adopted with “no evidence” it seems.
Yes, yes, I know why New Zealand was able to do something other countries couldn’t do. I’m just objecting to the idea that it didn’t have “strict non-pharmaceutical interventions”. It did.
Both citizens and non-citizens were prevented from entering the country for years. In most places almost every business was shut down and people had to stay home for a month in early 2020, and then restrictions were gradually loosened over several months; there might be some other countries that did a lockdown that extreme but none come to mind. They later did another lockdown in Aukland, very strict for a couple of weeks and gradually looser over the subsequent months.
So, no, New Zealand is not an example of countries that didn’t have strict NPIs. It’s the opposite: it’s a country where strict NPIs saved thousands of lives.
OK, so then maybe we learned one month or so can be ok if you can also control the border. Then when you open the border, the worst of the hysterical medical and public health responses have already run their course in other regions. But everyone gets infected anyway when you open up.
That is essentially the original quarantine idea at the city level from ~500 years ago. I could see that narrative making sense.
Anon,
New Zealand did much more than “one month of lockdown.”
Seems like you have forgotten all about Peru and other places where there were no NPI to speak of. Or, for that matter, Italy, or New York City.
You’ve proven to be impervious to facts on this issue, so I won’t bother trying. But for anyone else who is reading these comments and has somehow forgotten what happened during 2020 and early 2021: places that tried something resembling “business as usual” experienced very high mortality, almost all of it due to COVID.
I don’t want to be seen as arguing that COVID responses in all high-NPI countries or states were reasonable, which was definitely not always the case. But the idea that most of the mortality was due to the COVID response rather than COVID itself is nonsense.
My facts are simply the news telling me New Zealand was normal for most of 2020, heres another:
https://www.theguardian.com/world/2020/jun/09/a-beautiful-day-new-zealand-handshakes-and-hugs-its-way-back-to-pre-covid-19-life
I have no problem dismissing everything in the news as BS, is that what you are telling me to do? In general I don’t know what really went on in other countries.
I do know in the US that positive covid tests meant inept medical and public health interventions though. NYC mortality dropped by an order of magnitude after they stopped the ventilator thing the media and public health agencies were all clamoring for!
It’s hard for me to believe that people are still having these types of arguments about the effects of NPIs on COVID outcomes, least of all at this site.
It’s an extremely complex issue that involves many, many complex confounding variables across contexts. It also involves assumptions about the counterfactual of what would or wouldn’t have happened absent NPIs in specific locations – speculation for which there is little evidentiary support but which at least necessarily requires an explication of the assumptions being made. Just determining the effect of NPIs or lack thereof in a place like New Zealand or Sweden, in itself, is incredibly complex – but assuming that you can generalize from those context to other contexts that are fundamentally dissimilar in so many ways – sorry to argue from personal incredulity but it boggles my mind that smart people think they can do so at some meaningful level without doing just a ton of work first.
I think it’s entirely worthwhile to analyze the question of the costs and benefits of COVID NPIs, in various contexts. But I don’t see any worth in facile speculation except in the sense that sometimes it feels good to confirm biases.
There is really nothing complex. Preventing elderly from seeing family/friends, telling them to be afraid all day on tv if they have shortness of breath, and so on is abuse. It makes vulnerable people die sooner. And covid was widespread in nursing homes anyway, so the only options were covid or covid + abuse.
No one would voluntarily allow their own loved ones to be assigned to a treatment group like that in an RCT. The only complexity is in how people will justify their own selfish hysterical behavior. Will it be anger, denial, bargaining, etc?
The correct response is to take measures so it never happens again.
Anon,
Right, New Zealand largely avoided the negative effects of COVID. You claim that is because they did not have substantial non-pharmaceutical interventions. I claim that it is because they did have substantial non-pharmaceutical interventions. One of those is wrong and one of those is right.
New Zealand closed their borders for many months, and large parts of the country went into almost complete lockdown for weeks at a time, more than once. Your denial of the effectiveness of those measures is absurd.
Anoneuoid –
> There is really nothing complex. Preventing elderly from seeing family/friends, telling them to be afraid all day on tv if they have shortness of breath, and so on is abuse. It makes vulnerable people die sooner.
What’s complex is asserting a net effect of NPIs versus no NPIs. It necessarily requires counterfactual assumptions about what would have happened NPIs. That’s obviously very complex. Not only that, even if you were to make reliable conclusions about the impact of NPIs in one context, generalizing to another is very complex.
I’m talking about fundamental principles of epidemiology here. Going from correlation to causation is complex.
I lived in a Hasidic Jewish neighborhood in NY during March 2020. This was a population that broadly, depending on the rabbi, did not shut down or respect any NPIs, or even believe very strongly in the virus. There was, nonetheless, a massive spike in at-home deaths. The funeral homes were overcrowded, with body bags piled up in the hallways. Tents were set up in the streets to hide the dead, and the blare of ambulances was a constant drone. This discussion is absurd.
Here’s a statement that should be uncontroversial:
The fewer people who get COVID pre-vaccination the fewer bad effects the COVID virus will cause, and the less time spent in high stress social distancing situations, the less bad effects high stress social distancing situations will cause.
NZ did well because it was able to virtually eliminate the virus while having relatively short duration of personal intense social distancing (as a nation, isolating the borders went on for a long time, but individuals didn’t have to stay home).
Anoneuoid is annoying because he never seems to acknowledge that catching the virus was extremely dangerous *even after the excessive ventilation* up until the point where widespread immunization reduced the severity of illness.
And I agree that it’s annoying. But he’s not wrong when he says that high stress personal NPI activities had bad effects on people.
IMHO the social distancing we did kept the death toll from being 10-20M in the US which it easily could have been if the “just open up everything and try for herd immunity” crowd from middle of 2020 had gotten their way. Delaying COVID until after vaccinated was a huge huge win. I suspect Anoneuoid doesn’t agree, but if that’s the case I think he’s deluded.
The point of all the NPIs was always to keep the numbers down until vaccination could reduce the severity of illness.
Daniel –
> Tthe less time spent in high stress social distancing situations, the less bad effects high stress social distancing situations will cause.
I certainly agree that should be non-controversial. Unfortunately some people are reluctant to acknowledge that reality because of how NPIs have become political. Acknowledging what you say seems to be giving in to the “Great Reset” and “Plandemic” narratives – where NPIs were initiated by statist bureaucrats in cahoots with Big Pharma to keep the common folks down and suppress freedom-lovers for the sake of destroying capitalism and denying Trump his rightful status as the leader of the free world. That’s not an excuse for not acknowledging the potential harms proximally caused by NPIs, but I can understand that reluctance.
> But he’s not wrong when he says that high stress personal NPI activities had bad effects on people.
I think in a trivial sense he’s not wrong. In any meaningful sense, it’s being willfully obtuse.
Of course some NPIs can be the direct cause of harm along a number of vectors. But the critical question, imo, is whether they differentially caused harm in comparison to the harms caused by the pandemic in itself. And also, relatedly, whether they differentially caused harm in comparison to what would have happened had they not been implemented. Saying that NPIs cause harm is like saying that airbags and seatbelts cause harm. What I find “annoying” is that smart people treat these arguments as if it’s easy to attribute causality, and as if you don’t need to assess the differential effects by considering the potential counterfactual scenarios. Why do they engage in such facile reasoning? Yes, I find it annoying.
somebody: thanks, very nice example.
Joshua: yes I agree with everything you said, there was no better choice than to do some level of NPI, the right level was up for discussion, in my opinion in many cases we did too little, for example allowing 2020 Sturgis rally was certainly the direct cause of thousands to maybe even hundreds of thousands of deaths… In some cases we may have done too much … but I don’t think that was common. One of our commenters here Cory Yanofski was cited $500 or something like that for walking his dog in an empty park. https://ottawacitizen.com/news/local-news/britannia-man-fined-880-while-walking-dog-through-britannia-park that was CERTAINLY insane.
Ugh, correct spelling was Corey Yanofsky I do tend to get the spelling confused because Cory Doctorow has no “e” in his first name and I went to school with a guy in high school whose name was Yanofski with an “i”
I suspect a better comparison than New Zealand for understanding the influence of NPIs is the state of Victoria, or more specifically the city of Melbourne, Australia. Large population (~ 5 million), fairly high density, and very severe restrictions in place for a long period of time. The result was below-average statewide mortality through 2020 and only slightly increased mortality (3.4%) in 2021. (See https://www.abs.gov.au/articles/measuring-australias-excess-mortality-during-covid-19-pandemic-until-first-quarter-2023)
Oh, sure, there was plenty of bad decision-making around the response, and sometimes just plain nuttiness.
The CDC took far too long to acknowledge that just about all of the danger was in airborne transmission; readers of this blog seemed to recognize that months before the CDC did.
I have a friend who was not allowed to visit her father in the nursing home for months. She would fly east and spend a week sitting outside the window every day, looking in and talking to him on the phone because they weren’t even allowed to open the window. Presumably that policy was intended to protect staff, not to protect her father, since he would certainly have preferred to have close personal contact with her even if that shortened his life by a few months.
And once it was clear that few children are at high risk themselves, and that infected children are unlikely to infect adults, schools should have been able to reopen with some reasonable precautions. Yes, teachers would have been at elevated risk that way, but we could have paid them hazard pay, and allowed those at greatly elevated risk (elderly, immunocompromised, whatever) to take leave for the duration of the pandemic.
As a society we are downright weird about what risky behavior is and is not allowed. As I’ve mentioned before on this blog, challenge trials would have been extremely useful early in the pandemic. Get 10000 volunteers, expose them in groups of 20 to different COVID-infected people for different amounts of time, get some data on how long it takes to pass on the infection and how much variation there is from one infected person to another. Have half of them wear N95 masks and see how much difference there is. Stuff like that coulda and shoulda happened in the first six months. Yes, even if all of the volunteers were in their twenties and thirties some of them would have had some bad health outcomes; I understand why bioethicists don’t like this sort of thing. But those people can volunteer to join the army, and get sent to Afghanistan or Iraq or wherever else, and some of them will have bad outcomes that way too! Or you can become an ER doctor or nurse and take your chances that way.
I could go on and on. There’s lots of stuff in the world I disagree with, and some of those things relate to COVID response. Thinking through what decisions ended up being good and bad would be well worth doing. But you can’t look at outcomes, you have to look at the decision-making process: the next pandemic will involve different hazards and different facts will be known. Lives could have been saved by ‘proning’ hospitalized patients earlier, but nobody knew that at the start. It’s worth looking into how long it took word to get around, and whether that practice could have become standard much earlier in the response; I have no idea but if the answer turns out to be “the news spread like wildfire as soon as the evidence was pretty strong, and the practice was widespread within weeks” then, well, tough luck for the people who got sick and died before this became common practice but that doesn’t indicate that anything went wrong with the response.
Anyway I strongly agree that some elements of the response were not good by any measure. But to argue that all non-pharmaceutical interventions were either useless or harmful, as Anon does and some others do…that’s utterly wrong.
I guess Daniel, somebody, and I are preaching to the choir though. Anon isn’t going to change his mind, and everyone else agrees with us already!
Daniel, I agree it is very annoying to those on this blog. But how about when you attribute deaths to covid, there should be some accounting for inept response as well.
Show me one publication that does this. Then we can start there with all the problems in interpreting the results. The next step will obviously be applying the same standard to studies you happen to agree with.
I have said before, this covid response is not at all exceptional. In fact they followed the standard health/medical research protocols and the problems I am pointing out are the tip of the iceberg.
“Some of the excess mortality in 2020 vis a vis 2019 was death from covid, death from covid-related – drug overdose, etc.) … Statistics 101 says that a study should have already been done looking at this” Yes, very many such analyses, I know some from Canada such as https://www.cmaj.ca/content/194/21/E741 But because COVID is always changing, infection control measures are changing, and treatment of the sick is always changing, its not trivial to control for a single variable and show that this or that policy has this or that effect. And there are lots of ways to cheat, the Swedish authorities have been accused of overestimating the expected level of mortality to make their laissez-faire policy look better, and many governments worked to reduce case counts (not cases) in 2021/2022.
Deb –
> Ventilators almost certainly decreased life expectancy.
Perhaps assuming that correlation = causation is sometimes sub-otpimal?
https://gidmk.medium.com/did-ventilators-kill-people-during-covid-19-c07283933865
Deb –
> Ventilators decreased life expectancy
Argument by assertion is so persuasive.
A quick google turned up this: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10079311/
Please do not use this blog to spread conspiracy theories. There are enough places on the internet for this sort of thing already.
Taiwan had advance warning in the form of the 2002-2004 SARS outbreak, which left a lasting impression on all Taiwanese people and rearranged their disease control policy.
The vice-president (now premier) who led the COVID response in Taiwan is an epidemiologist
.
Not only that, but it’s absurd to look at the results in Taiwan to make broad parallels to what would or wouldn’t work in the US. Not only because Taiwan is an island nation, but also because in contrast to the US, the populous tends have a very different view on the idea there’s some some kind of basic zero sum balance between “personal freedom” and thinking of the greater public good. For example, that attitudes towards wearing masks is completely different in Taiwan than in the US. They executed contact tracing and quarantining on an entirely different scale than the US.
Can anyone imagine something like this being implemented in the US with so many “freedom fighters” running about to make sure everyone is free from tyranny and will never have to wear a mask?
https://www.bbc.com/news/business-60461732
Population, populous. I hate it when I do that.
From your comments about strong immune systems and supplements (ie vit D), you don’t have a good grasp of biomedical issues, but this – lives saved by ivermectin and hydroxychloroquine?
https://www.sciencedirect.com/science/article/pii/S075333222301853X
this link estimates that about 17000 people died due to ineffective treatment with hydroxychloroquine.
The best thing for your immune system is to prime it with a vaccine. You want a balanced immune system not a “strong” one unless you are a fan of autoimmune disease.
The HCQ was not ineffective. They were overdosing people by giving twice or more the usual dose (based on in vitro studies), which causes methemoglobinemia (basically oxidized iron in the hemoglobin). This was not being tested for, despite being a known effect of chloroquine overdose. It has the same weird symptoms as the early reports of severe covid, and is treated with vitamin C.
At first it looked like covid itself was causing the methemoglobinemia, but the reports of strange symptoms seemed to go away when that fad passed. Maybe it was both, who knows? There seems to be no interest in figuring out what was going on with that “happy hypoxemia” phenomenon.
https://en.wikipedia.org/wiki/Methemoglobinemia
I need to ask. Would anyone be interested in learning more about the HCQ-methemoglobinemia topic from peer reviewed medical research that was published both as it was happening as well as more recent recaps?
Because it doesn’t seem like anyone cares to figure out what actually happened.
I’m not interested in your theory about methemoglobinia. But I would like to know which peer reviewed literature you look to as evidence for this statement:
> The HCQ was not ineffective
Its in the link I responded to… Overdosing people on HCQ looks like it *increased* mortality by ~10%. How is that “ineffective”? It was actively harmful.
Now, if they had given normal doses along with azithromycin as originally suggested, who knows? It was never studied. But we also learned later that ~30% of people who died “from covid” actually died from bacterial infections they picked up in the hospital. So seems plausible it would have helped.
Anoneuoid –
So if I get you right, now you’re saying that this:
> > The HCQ was not ineffective
is ungrounded, and you don’t have any evidence that HCQ was not ineffective?
And I’ll add this:
> ~30% of people who died “from covid” actually died from bacterial infections they picked up in the hospital
Do you have peer reviewed research that shows that 30% of people who died from COVID actually died from bacterial infections they picked up on a hospital?
I’m particularly interested in those people who died from covid and never visited a hospital yet apparently died from a bacterial infection they got at a hospital. How does that work?