Paul Campos writes:
Probably the biggest public health success in America over the past half century has been the remarkably effective long-term campaign to reduce cigarette smoking. The percentage of adults who smoke tobacco has declined from 42% in 1965 (the first year the CDC measured this), to 12.5% in 2020.
It’s difficult to disentangle the effect of various factors that have led to this stunning decline of what was once a ubiquitous habit — note that if we exclude people who report having no more than one or two drinks per year, the current percentage of alcohol drinkers in the USA is about the same as the percentage of smokers 60 years ago — but the most commonly cited include:
Anti-smoking educational campaigns
Making it difficult to smoke in public and many private spaces
Increasing prices
Improved smoking cessation treatments, and laws requiring the cost of these to be covered by medical insurance
I would add another factor, which is more broadly cultural than narrowly legal or economic: smoking has become declasse.
This is evident if you look at the relationship between smoking rates and education and income: While 32% of people with a GED smoke, the percentages for holders of four year college degrees and graduate degrees are 5.6% and 3.5% respectively. And while 20.2% of people with household incomes under the $35,000 smoke, 6.2% of people with household incomes over $100,000 do.
All worth noting. Anti-smoking efforts are a big success story, almost such a bit story that it’s easy to forget.
The sharp decline in smoking is a big “stylized fact,” as we say in social science, comparable to other biggies such as the change in acceptance of gay people in the past few decades, and the also-surprising lack of change in attitudes toward abortion.
When we have a big stylized fact like this, we should milk it for as much understanding as we can.
With that in mind, I have a few things to add on the topic:
1. Speaking of stunning, check out these Gallup poll results on rates of drinking alcohol:
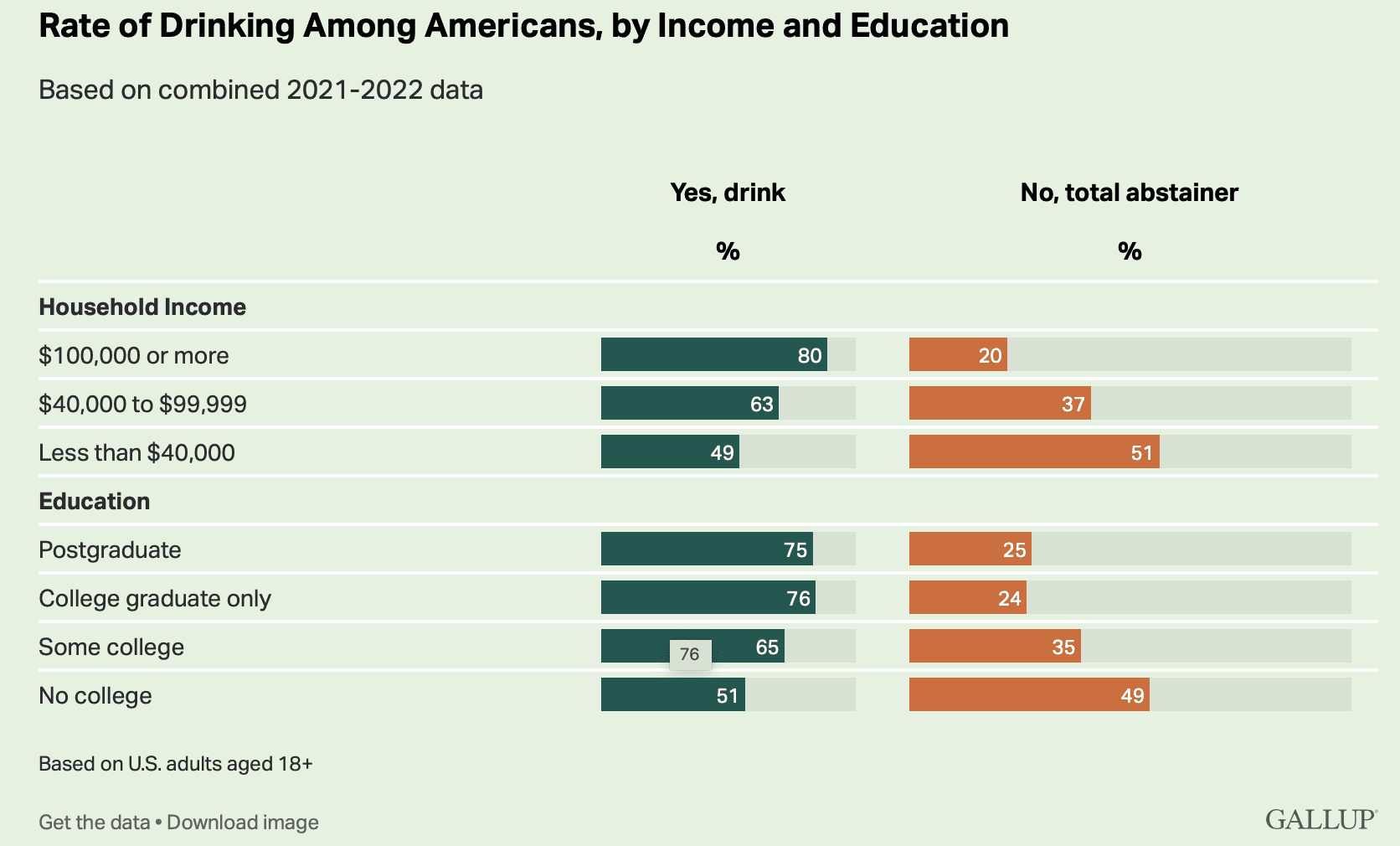
At least in the U.S., rich people are much more likely than poor people to drink. That’s the opposite of the pattern with smoking.
2. Speaking of “at least in the U.S.”, it’s my impression that smoking rates have rapidly declined in many other countries too, so in that sense it’s more of a global public health success.
3. Back to the point that we should recognize how stunning this all is: 20 years ago, they banned smoking in bars and restaurants in New York. All at once, everything changed, and you could go to a club and not come home with your clothes smelling like smoke, pregnant women could go places without worrying about breathing it all in, etc. When this policy was proposed and then when it was clear it was really gonna happen, lots of lobbyists and professional contrarians and Debby Downers and free-market fanatics popped up and shouted that the smoking ban would never work, it would be an economic disaster, the worst of the nanny state, bla bla bla. Actually it worked just fine.
4. It’s said that quitting smoking is really hard. Smoking-cessation programs have notoriously low success rates. But some of that is selection bias, no? Some people can quit smoking without much problem, and those people don’t need to try smoking-cessation programs. So the people who do try those programs are a subset that overrepresents people who can’t so easily break the habit.
5. We’re used to hearing the argument that, yeah, everybody knows cigarette smoking causes cancer, but people might want to do it anyway. There’s gotta be some truth to that: smoking relaxes people, or something like that. But also recall what the cigarette executives said, as recounted by historian Robert Proctor:
Philip Morris Vice President George Weissman in March 1954 announced that his company would “stop business tomorrow” if “we had any thought or knowledge that in any way we were selling a product harmful to consumers.” James C. Bowling . . . . Philip Morris VP, in a 1972 interview asserted, “If our product is harmful . . . we’ll stop making it.” Then again in 1997 the same company’s CEO and chairman, Geoffrey Bible, was asked (under oath) what he would do with his company if cigarettes were ever established as a cause of cancer. Bible gave this answer: “I’d probably . . . shut it down instantly to get a better hold on things.” . . . Lorillard’s president, Curtis Judge, is quoted in company documents: “if it were proven that cigarette smoking caused cancer, cigarettes shoudl not be marketed” . . . R. J. Reynolds president, Gerald H. Long, in a 1986 interview asserted that if he ever “saw or thought there were any evidence whatsoever that conclusively proved that, in some way, tobacco was harmful to people, and I believed it in my heart and my soul, then I would get out of the business.”
6. A few years ago we discussed a study of the effects of smoking bans. My thought at the time was: Yes, at the individual level it’s hard to quit smoking, which might give skepticism about the effects of measures designed to reduce smoking—but, at the same time, smoking rates vary a lot by country and by state, This was similar to our argument about the hot hand: given that basketball shooting success rates vary a lot over time and across game conditions, it should not be surprising that previous shots might have an effect. As I wrote awhile ago, “if ‘p’ varies among players, and ‘p’ varies over the time scale of years or months for individual players, why shouldn’t ‘p’ vary over shorter time scales too? In what sense is “constant probability” a sensible null model at all?” Similarly, given how much smoking rates vary, maybe we shouldn’t be surprised that something could be done about it.
7. To me, though, the most interesting thing about the stylized facts on smoking is how there is this behavior that is so hard to change at the individual level but can be changed so much at the national level. This runs counter to currently-standard individualistic theories in social science in which everything is about isolated decisions. It’s more of a synthesis: change came from policy and from culture (whatever that means), but this still had to work its way though individual decisions. This idea of behavior being changed by policy almost sounds like “embodied cognition” or “nudge,” but it feels different to me in being more brute force. Embodied cognition is things like giving people subliminal signals; nudge is things like subtly changing the framing of a message. Here we’re talking about direct education, taxes, bans, big fat warning labels: nothing subtle or clever that the nudgelords would refer to as a “masterpiece.”
Anyway, this idea of changes that can happen more easily at the group or population level than at the individual level, that’s interesting to me. I guess things like this happen all over—“social trends”—and I don’t feel our usual social-science models handle them well. I don’t mean that no models work here, and I’m sure that lots of social scientists done serious work in this area; it just doesn’t seem to quite line up with the usual way we talk about decision making.
P.S. Separate from all the above, I just wanted to remind you that there’s lots of really bad work on smoking and its effects; see here, for example. I’m not saying that all the work is bad, just that I’ve seen some really bad stuff, maybe no surprise what with all the shills on one side and all the activists on the other.
Given that in a sense, you don’t have to “change” (existing) individual or society-wide behaviors to reduce smoking rates if people never start smoking to begin with, seems to me to some extent focusing on change of individual behaviors versus change in behaviors society-wide may underestimate a key component.
How has the rate of smoking among young people changed, and what are the characteristics of the change (e.g., is there a socio-economic signal)?
What might the likely causal factors be, if rates of smoking rates in young people changed dramatically? I suspect that effects from policies there might be less, or at least more indirect (with a likely exception of advertisement-related policies)?
Here’s a link to smoking rates by age group: https://www.ncbi.nlm.nih.gov/books/NBK294302/figure/ch13.f11/. Your point is one that many economist have noted. In the past, some of the public response to an increase in tobacco taxes is people saying that it won’t get people to quit. I don’t know how true that claim is (last time I read the literature on that was about 10 years ago, and there was enough debate for me not to come to a firm conclusion), but what has been observed is a decrease in people starting to smoke when tobacco taxes are raised. This seems like something aimed at the individual that has really worked.
That being said, as Andrew mentioned, choices are embedded in social context and the choices of those around you will have an impact on how you choose. I don’t see it as anything mysterious. Most people want to fit in and are willing to do so at some cost. But individuals (not groups) do make choices, and that’s why we see change.
A data point: I asked my college-attending grandchild what percentage of her classmates smoke, and she estimated under 5%. I asked her what percentage vape, and she estimated 60%. Smoking may be disappearing, but nicotine consumption is still high.
Jesus. Just googled a bit. Even if 60% us an overestimate, more official estimates are way higher that I eould have guessed. As of I needed more proof that I’m an old fogey.
Here’s a small US data set, self-reported, from one US college (and a German school with much lower rates) that’s two years old at 40%, and we know it’s increased since then.
https://www.pulmonologyadvisor.com/home/topics/smoking/a-third-of-college-students-vape-and-many-vaped-more-often-during-pandemic/
Better data, I think
https://www.statista.com/statistics/1126218/us-college-student-tobacco-use-by-product/
Andrew wrote this:
“All worth noting. Anti-smoking efforts are a big success story, almost such a bit story that it’s easy to forget.”
I think this was meant: “All worth noting. Anti-smoking efforts are a big success story, almost such a big story that it’s easy to forget.”
I would guess there are a lot of differences between income/education groups that may account for some of these results. Some that would be worth looking in to: hours worked, age distribution, share of income spent on smoking and alcohol, urban/rural divide, religiosity.
> Then again in 1997 the same company’s CEO and chairman,…
Given it seemed like you were going chronologically and it would be surprising to me for anyone to have said anything like this in 1997 was this a typo, perhaps 1979?
Regarding alcohol consumption (which was referenced briefly in this article), there was a recent discussion on this blog, which I consider worth a reading: https://statmodeling.stat.columbia.edu/2023/09/03/how-many-americans-drink-alcohol-and-who-are-they/
Staying with the alcohol topic, I would like to echo Dale Lehman’s comment (https://statmodeling.stat.columbia.edu/2023/09/03/how-many-americans-drink-alcohol-and-who-are-they/#comment-2257534) from back then: The really interesting question is who drinks how much and how often, which the graph above cannot tell us.
Yes I think on alcohol in particular this is important. Some people are total abstainers for religious reasons, some because they are in “recovery” meaning that at one time in the past they drank daily (not an exact definition). So when I see those statistics I also want to know what the time frame for the total abstainer response is.
I do think the health messaging on alcohol has been much less clear, and of course there are no legal bans at bars or restaurants or even offices. BUT if the restaurants you eat at are fast food versus more expensive, yes probably there is an effective ban.
In my first professor job, one of the very senior faculty members had a small liquor cabinet in his office and would periodically invite people to have a sherry or whatever. I doubt this is as common as it used to be.
Each event has its own unique probability but you can plug in the average (arithmatic mean) instead to get the same overall observed frequency. Ie, the frequency of success is a summary statistic that can map to many different sets of probabilities.
With more info you could also say more, ie about the sequence. But at least using the average probability lets us say something about the phenomenon.
1) ADDICTION : For most, nicotine addiction ony works during adolescent brain development, within window ages 10-24.
https://twitter.com/JohnMashey/status/929835136564150273
This has annotated curves from Insitute of Medicante/National Academies report showing distribution of start-age years of adult smokers.
Almost no adult starts after age 24 and gets really addicted, and of coruse the tobacco co’s have known thsi for at least 4 decades.
RJ Reynold, ~1984, “The importance of younger adults” *really, meaning ages 12-18), 3 years before Joe CameL:
https://www.industrydocuments.ucsf.edu/tobacco/docs/#id=jzyl0056
Volume: get em young
Market Share: get em before the others do, first brand is sticky.
UCSF’s Industry Documents Library has ~90M pages of internal tobacco company documents for starters, plus some from other industries,
basically companies that privatize profits and socialize damages to health.
https://www.industrydocuments.ucsf.edu
2) QUITTING:Both nicotine sensitivity and brain development vary (by genetics and other issues), but to some extent addiction level ~ amount of exposure during most intense adolescent brain development. If someone tells me they quit cold turkey, I ask when they started. Most commonly, it was light smoking socially during college. I’ve also heard examples where people said they started smoking heavily as teenager, but much rarer.
Mostly, if someone used a lot of nicotine during adolescent brain development, they’ll need multiple quit attempts to stop, and may not succeed.
3) INTERNATIONAL: as US/Canada/Europe/Australia,. etc cut back on smoking, Philip Morris split into Altria and PM International.
I think most countries have declined, slightly, but not all:
Indonesia: https://www.macrotrends.net/countries/IDN/indonesia/smoking-rate-statistics
That also has links to rates/charts for many other countures.
Egypt has bounced around: https://www.macrotrends.net/countries/EGY/egypt/smoking-rate-statistics
Congo has icnreased: https://www.macrotrends.net/countries/COG/republic-of-congo/smoking-rate-statistics
Many fothe countiers show declines from 2000-2018, then ~flat 2018-2020. I have no idea what that means.
(Low-funded) African health departments fight constant battles against tobacco co’s, especially given politican corrutpion.
I have no idea what “Many fothe countiers” means either.
Many of the countries
Yes, countries. I was surprised at the common pattern of slow descent until ~2018, then flat 2019-2020. Maybe COVID in latter part?
Oops forgot. I know of a few studies, such as this from 2008:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6879091/pdf/MPR-17-S16.pdf
H.-U. WITTCHEN,1,6 S. BEHRENDT,1,6 M. HÖFLER,1 A. PERKONIGG,1 R. LIEB,2,3 G. BÜHRINGER,4,5
K. BEESDO1 What are the high risk periods for incident substance use and transitions to abuse and dependence? Implications for early intervention and prevention
Fig 1 has 4 charts that compare Use, regular use and dependence (~addiction) for Females & Males, for Alcohol and Nicotine, by age. Summary: Most try alcohol, 60%(F), 80%(M) drink regularly, very few (F) graudate to dependency.
Nictoine: 70-80% try it, 50-60% become regular users, 20-30% become dependent.
Figure 3 does same for Cannabis and Other Illicit Drugs.
I don’t have this one (Paywalled), but abstract is interesting:
Transitions from first substance use to substance use disorders in adolescence: Is early onset associated with a rapid escalation?
S. Behrendt a, H.-U. Wittchen a, M. Höfler a, R. Lieb b c, K. Beesdo
https://www.sciencedirect.com/science/article/abs/pii/S0376871608002470
Smoking is powerfully addictive. Stories are told of concentration camp inmates trading food for tobacco. I tried to be the stern MD, but I don’t recall anyone quitting because I told them. Every MD of my vintage can recollect people holding a cigarette to their tracheostomy. I would attribute much of the change to social pressures like no smoking in bars and no smoking by role models in entertainment.
I smoked in college and medical school. My quitting was an up and down process with periods of substitution (pipe) and abstinence with relapses. I once relapsed after about six months of abstinence. Social pressure did the trick.
Rationality doesn’t explain everything about human life.
Cessation experts I’ve talked to say addiction ~combination of
1) physiological, i.e. Google: NAChR upregulation,
Ie the changes that repeated nicotine exposure causes in nicotinic acetylcholine receptors.
2) social/habitual
I made at least ten serious attempts to quit over 35 years.
Seems to me a massive overlooked factor in medical circles – I don’t think I’ve ever even seen it mentioned in any medical discussion about nic or smoking – is that nicotine is an extremely powerful stimulant. If you want to drive for 36 hours and stay alert, cigs are *far* more effective than coffee. When people say they smoke to “relax”, what they mean is that they smoke when they’re tired and stressed, and nic the powerful stimulant eases the tiredness thereby easing the stress. My bet is that what gets people hooked is that the craving for this solution to being tired develops extremely quickly without them recognizing that they’re relying on a chemical stimulant to keep going. People attribute the “relaxing” sensation to the act of smoking itself, rather than to nicotine as a stimulant.
This suggests the reason why today smoking and nic use is more prevalent among lower income people: they’re more likely to be performing physical labor and thus need a more powerful stimulant than, say, an accountant would need.
Regarding why fewer people smoke today than in the past: seems pretty obvious! Today it’s well known to be dangerous. My first years in school were in California. I’ll never forget the materials we got in school informing us of the dangers of heroin. While I tried many drugs in my youth, I never touched or considered using heroin because those materials scared the hell out of me.
There are also some benefits to smoking too. It helps many people with Schizophrenia and possibly some other Psychiatric issues, not to mention relief at high altitudes. Additionally, simply a ritual of holding a cigarette between one’s fingers or lips is what makes it hard to stop. They miss a sensation of that tactile habit. Although I never smoked, I don’t believe it is as bad as it has been advertised. In the extreme cases, sure, but it’s quite complicated. There are whole countries with very high smoking rates and they still live like the rest, on average. As I type this, a large chunk of CA is breathing smoke 24/7, sometimes weeks on end. How would one disentangle exposure to other environmental toxins, mostly smoke/fumes/cars/etc. from that of 20 cigarettes or so? It takes an hour a day perhaps, to smoke a pack, but I’m breathing in all the toxic wildfire smoke and automobile smog too, and it never stops. What if a person lives in the woods in relatively clean air, but smokes a pack a day. Are they worse off than an urban non-smoker?
Navigator:
If people want that “ritual of holding a cigarette between one’s fingers or lips,” I strongly recommend for reasons of health that they do so without lighting up. Or they could use a straw or something like that instead.
I also recommend environmental policies that would reduce the level of smoke in the air.
In addition, if someone lives in the woods and wants that ritual of holding a cigarette between one’s fingers or lips, I strongly recommend for reasons of health that they do so without lighting up. Or they could use a straw or something like that instead. My advice here still works for people who live in the woods.
I imagine there are other ways for people to handle psychiatric issues and relief at high altitudes, but if smoking is the only way for them to handle it, then, yeah, maybe it’s worth having a higher risk of all sorts of diseases. I can’t make that tradeoff for them.
Navigator –
> Although I never smoked, I don’t believe it is as bad as it has been advertised. In the extreme cases,
I think the connection between those two sentences should be considered.
I smoked for quite a few years. It negatively affected my health in numerous ways. It’s hard for me to imagine how it wouldn’t.
> It helps many people with Schizophrenia and possibly some other Psychiatric issues.
My brother was a schizophrenic. I can assure you that incredibly high rates of cigarette smoking was harmful to his health.
> It takes an hour a day perhaps, to smoke a pack, but I’m breathing in all the toxic wildfire smoke and automobile smog too, and it never stops.
There’s quite a bit of research that shows a correlation between risk for harms to children and living in households where caregivers smoke. (it could all be wrong but I tend to think that’s improbable). Living in a house with people who smoke is way less exposure that one hour a day of smoking. Yet it seems to have a significant impact.
As does living in heavily polluted areas. Obviously, as Andrew points out, there’s nothing mutually exclusive about the harms from smoking and the harms from pollution.
Just to correct that.
My brother had schizophrenia (I don’t like that I wrote my brother was a schizophrenic, as if he wasn’t far more than just that).
Am I right that you are describing “scale” problem similar to what is commonly reported in ecology?
I only follow social sciences as a “hobby”, but it seems to me that the problem you describe here is a matter of temporal scale. That is: you could easily (in principle) estimate the effect of policies on people’s success in quitting smoking, and/or in spontaneous rates of smoking cessation, if you had appropriate experiments running for decades. That would allow linking the large scale patters (the changes in smoking prevalence at the state or county level) to causal drivers at the individual level. However, those experiments are practically or financially impossible to conduct.
This issue seems similar to what happens in ecology, arising from the mismatch between macro- and population-ecology. Ecology has seen a deluge of large scale data – mostly species distribution data. These data show, for example, how species distributions are associated to certain levels of average precipitation and temperature. Intuitively, these associations should reflect physiological processes, such as adaptations to frost. However, linking these “average patterns” to causal drivers at the population or physiological level is – euphemistically speaking! – quite hard. For example, at the individual level, the effects of year-to-year changes in climate on individuals tends to be extremely small, and this signal gets swamped by the myriad other factors that determine the performance of individuals on a year-to-year basis. In this case, just as in the case of smoking cessation, estimating the causal processes at individual level (the relevant scale) is practically hard, but of fundamental importance to the subject.