Paul Alper points to this fun news article by Andrew Van Dam, who runs the “Department of Data” column for the Washington Post. Van Dam writes:
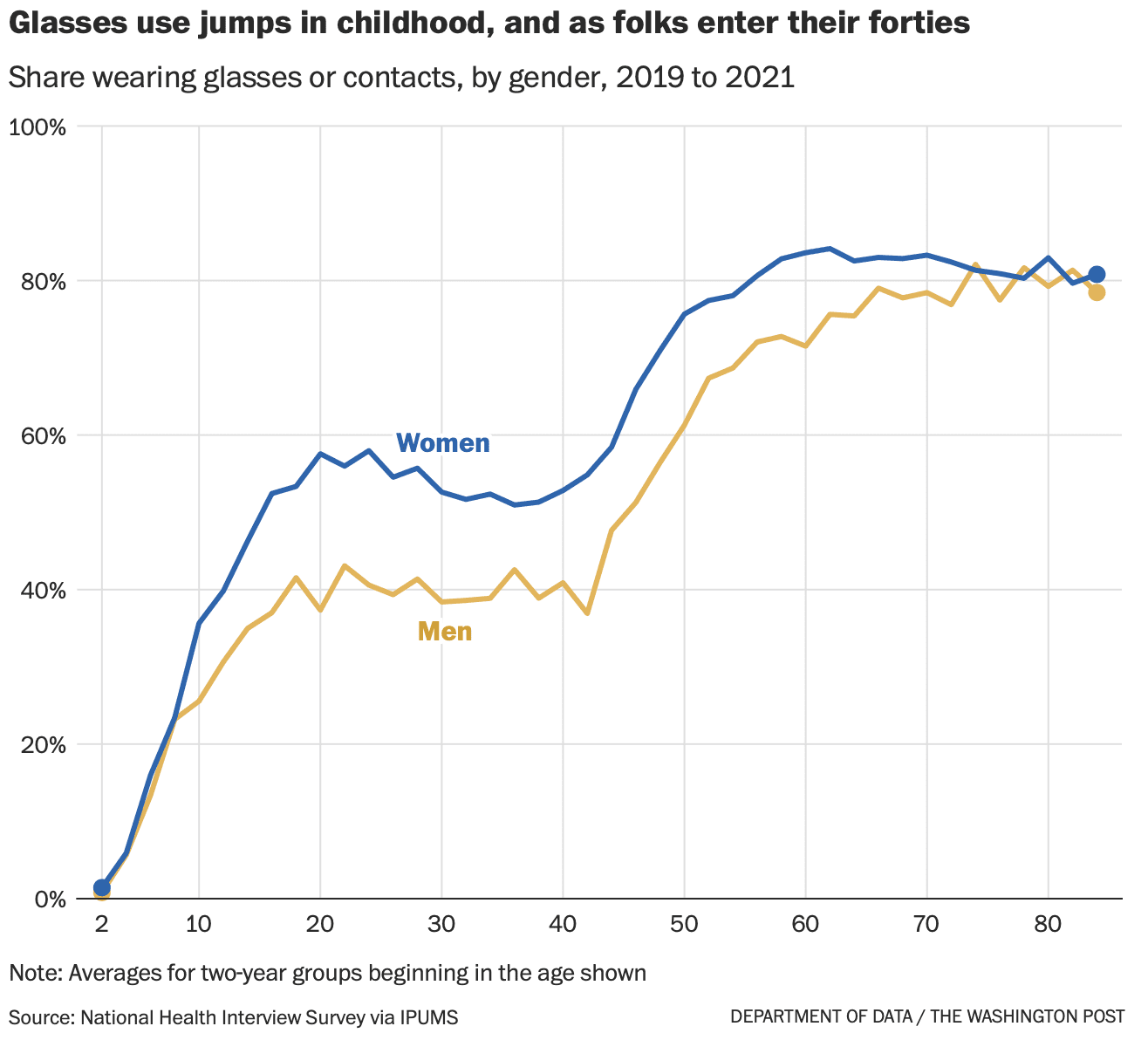
According to our analysis of more than 110,000 responses to the National Health Interview Survey conducted by the Census Bureau on behalf of the National Center for Health Statistics, 62 percent of respondents said they donned some form of corrective eyewear in a recent three year-period. . . .
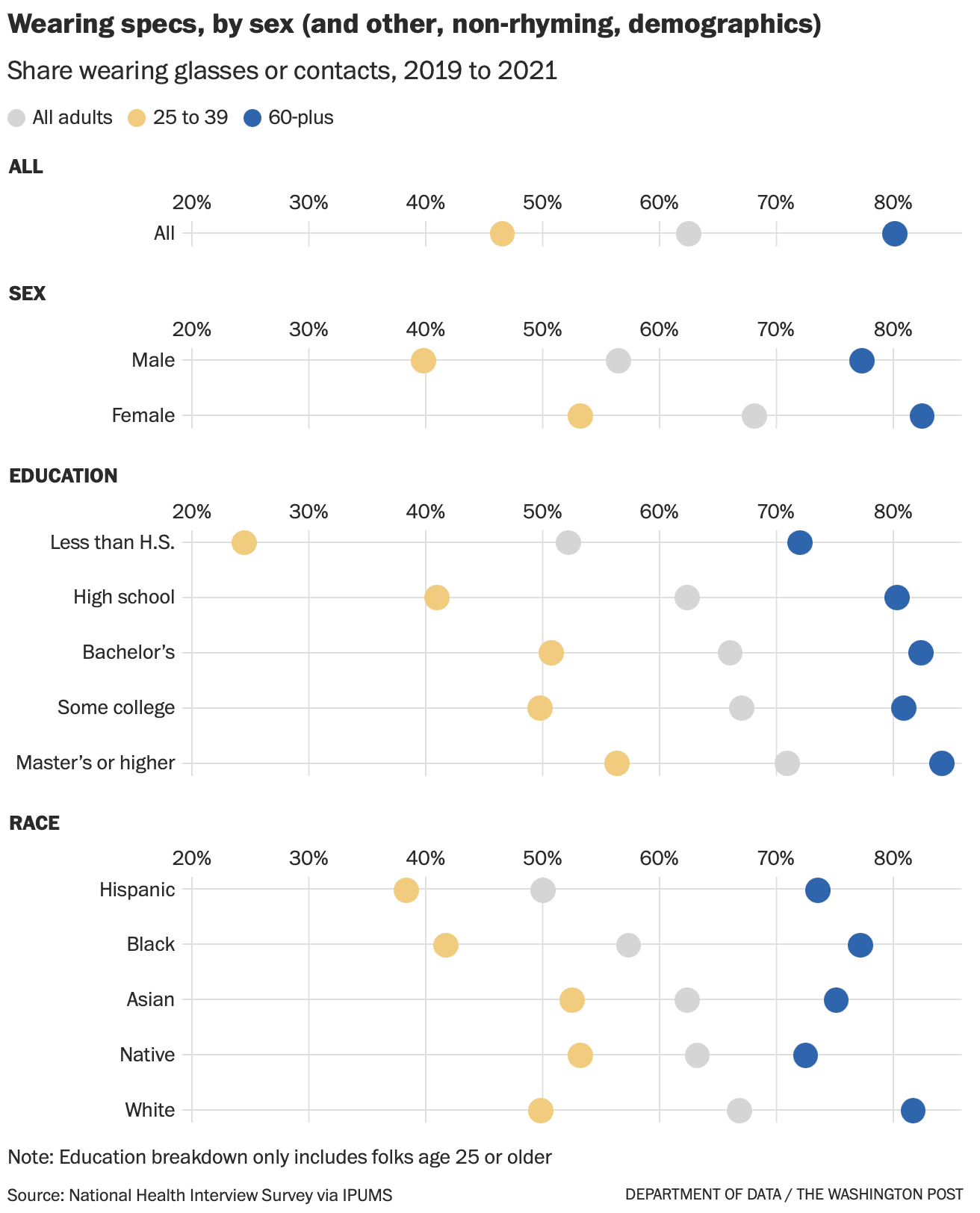
The ubiquity of eyeglasses in your personal universe will change depending on whether you’re hanging out with young legal workers (ages 25 to 39) or your friends who work in agriculture or construction. That’s because the legal workers are more than twice as likely to wear glasses.
What’s actually going on here? If good vision is hereditary, as we assume, how could your occupation determine your need for vision correction? . . . we called eye-data expert Bonnielin Swenor, director of the Johns Hopkins Disability Health Research Center. Swenor pointed us to her friend and colleague, Johns Hopkins Wilmer Eye Institute pediatric ophthalmologist and researcher Megan Collins, who appears to know everything about eyeballs. . . .
It turns out that, yes, myopia [nearsightedness] is on the march. In a 2009 JAMA Ophthalmology publication, National Institutes of Health ophthalmologists found that the prevalence of myopia had increased from 25 percent of the population age 12 to 54 in 1971 and 1972 to 42 percent of people in that age range in 1999 to 2004. The study was based on thousands of physical exams conducted for the National Health and Nutrition Examination Survey. . . .
Swenor and Collins explain that while kids may not have changed, the world around them sure has. And key changes in the way kids grow up — many associated with urban living and consumer technology — have been hard on the eyes. . . . According to a review of myopia research, spending time outdoors is one of the best things a kid can do for healthy eye growth. . . . Outdoor light may help your eyes grow, and being outside gives your eyeballs more opportunities to flex their muscles by focusing on distant objects. While data is surprisingly scarce, available evidence suggests kids may spend less time outdoors than they did a generation or two ago. . . .
Myopia has risen even more rapidly in East Asia, where countries have attempted sweeping remedies. A program in Taiwan, for example, encouraged students to participate in two hours of outdoor activity every day. After it began in 2010, researchers found in the journal Ophthalmology, Taiwan’s long rise in myopia went into reverse.
People also are more educated today, and many studies find that the more education you have, the more likely you are to be myopic. That correlation, of course, is probably related to the first two factors: To get a diploma or degree, you’ll probably spend more time indoors studying. . . . Education gaps often accompany much of the difference in myopia — and thus the glasses gap — among groups: Women are more likely to wear glasses than men. High earners are more likely to wear glasses than low earners. And Asian and White Americans are more likely to wear glasses than their Black and Hispanic compatriots.
Of course, myopia is not the only reason a more-educated person might be more likely to wear glasses. “There are a number of other factors that may be at play too,” Collins said, “including cost of eyeglasses, access to vision care, health literacy, or trust in the health-care system.” More educated Americans are also more likely to be doing jobs that require near work, such as typing or reading, and thus more likely to don reading glasses to compensate for the slow advance of presbyopia.
While myopia is an easily corrected annoyance for many of us, Swenor says its rising prevalence is also a bona fide public health issue. When the eyeball elongates, the stretching can damage the wall of your retina and cause permanent, non-correctible vision loss such as myopic macular degeneration. . . .


This is just great, an exemplar of newspaper science writing. Let me count the ways:
1. Lots of data graphics
2. Quotes with outside experts
3. This: “While data is surprisingly scarce, available evidence suggests . . .” I looooove this recognition of uncertainty.
This was so great that I added Van Dam’s column to our Blogs We Read page.
Dalam dunia perjudian online, kepercayaan dan keamanan merupakan dua aspek penting yang selalu dicari oleh para pemain. Ritogel, sebagai bandar togel online terpercaya, hadir untuk menjawab kebutuhan tersebut. Dengan komitmen untuk menyediakan lingkungan bertaruh yang aman dan adil, Ritogel telah menjadi destinasi utama bagi para penggemar togel di seluruh dunia.
Lots of interesting information here, but a couple of relevant points seem to be missing. There is no discussion of screening. Income, particularly in poorer countries, affects whether people are screened for vision problems, particularly at young ages. In fact, for some occupations (like farm labor), people may never get screened unless their eyesight is very poor. So, screening is likely not equal for different ages, different occupations, and different countries.
Related to this, it appears that the question on the NHIS that is being used is the following:
“Do you wear glasses or contact lenses?
* Read if necessary: Persons who wear glasses to read or to do other occasional tasks should answer yes to this question.”
I would answer yes if I worked outdoors and wore sunglasses. During my lifetime, I believe there has been a change regarding sunglasses – they are worn far more readily than when I was a child (for all age groups). If that conjecture is true, then part of the increase is not due to any change in eyesight, but due to changes in attitudes and practices. I find it hard to determine how much of the increased wearing of glasses over time, age, occupation, or education is due to changing eyesight or changing screening or changing practices.
It doesn’t appear that the article (paywalled so I didn’t read it) makes causative claims, so this is not a criticism per se. But I do think it is difficult to speculate about causes without additional information and there are such speculations in the excerpt above.
Dale wrote, “It doesn’t appear that the article (paywalled so I didn’t read it)…” Although Andrew claims I was the one who sent it to him, I have no memory of doing so. Because I have lived in the UK, what I do know, if only for the moment, is that the British vision term for the U.S. vision term, “nearsighted” is/was, “short-sighted” and with or without the hyphen, has/had a decidedly different, and exclusive non eyeball meaning in the U.S.
Scouting around on the web, I “see” that somehow, similar to vision as we get older, the British terminology for vision has shifted towards the American version.
Vox media has a good video on this:
https://www.vox.com/videos/2023/3/7/23629462/myopia-nearsightedness-glasses-elongated-eyeballs
The notion of non-correctible vision loss seems to come up whenever eye doctors want to sell something.
” If good vision is hereditary, as we assume, …” One way the article is not so great is biological understanding. Relatively few traits, like the pea traits studied by Mendel) are determined only by genes . The environment during development also matters, as the vision experts explained about vision, but the article does not explain that this is the normal case.
A data point. At a meeting of an undergrad computer nerd group (20 or so of us) at MIT in 1972, someone said: “Hey! Everyone close your eyes. Now calculate the probability that everyone in the room is wearing glasses. Now open your eyes.” Everyone was, of course, wearing glasses.
I really liked being nearsighted. Great for detailed work on things; just take off the glasses. Until I realized that it’s a really bad idea when you get to be 60 or so (sky high probabilitities of problems like detached retina and cataracts).
If you are at all nearsighted, you should be seeing an ophthamologist once a year, preferrably twice a year. Do not delay check ups more than a year. Whatever your age.
What’s interesting (in an anecdotal sense) is that pictures of ‘Andrew Gelman statististics glasses’ on Google ‘images’ that are identifiable as Andrew, I was served 7 with glasses and 1 without, for ‘Andrew Gelman statistics no glasses”, 3 without glasses and 7 with glasses.
Obviously, my sense of the value of a survey like mine is near zero.
Full disclosure – I wear glasses.
That all said, this was a great post Andrew to stimulate interest in what to do about spending too much time in front of a screen like I do, and not spending time to walk about looking at the beautiful mountains I live in. This is an indication that I should get out and about.
Mendelian Randomization analyses suggest that increasing education is contributing to the increasing prevalence of myopia: https://www.bmj.com/content/361/bmj.k2022
“Main outcome measures Mendelian randomisation analyses were performed in two directions: the first exposure was the genetic predisposition to myopia, measured with 44 genetic variants strongly associated with myopia in 23andMe, and the outcome was years in education; and the second exposure was the genetic predisposition to higher levels of education, measured with 69 genetic variants from SSGAC, and the outcome was refractive error.
Conclusions This study shows that exposure to more years in education contributes to the rising prevalence of myopia. Increasing the length of time spent in education may inadvertently increase the prevalence of myopia and potential future visual disability.”
I think the easy availability of $10 reading glasses (and 3-packs at Costco!) has made self-diagnosis easier for people in the US.
Health insurance with eye coverage also probably plays a role for those high income people.
The cited Ophthalmology study of the effect of outdoor activities on the rise of myopia in Taiwan caught my eye. I was curious how teachers managed to squeeze two extra hours of outdoor activities into the school day so I looked up the paper. I did not find a clear answer, but I found this “For the analysis by each 5-year period, the change in prevalence from 2011 through 2015 was -3.99% (50.11% declined to 46.12%). By comparison, during the previous 5-year period from 2006 through 2010, the change was +6.06% (43.04% increased to 49.10%). The total difference in these 2 periods before and after the policy intervention is 10.05% (3.99% þ 6.06%) in the 5 years from 2011 through 2015. Therefore, the reduction rate after intervention was approximately 20.5% over 5 years (10.05% / 49.1%) and 4.10% per year.
This seems to fit the description “big if true”. There is also an estimated regression equation (Table 2)
Y_t=-3406.43 +1.72 Time +1.54 Intervention -2.73 Intervention*Time
where Y_t is a proxy of the % of myopic students, Time is the number of years counting from 2000, and Intervention is the policy “encouraging” two hours of outdoor activities. This does not seem to make a lot of sense as the DV should be in the 40%-50% range. Please tell me if I had missed something. Thanks!
p.s. I cannot attach the paper here so I provide the link for pdf download instead https://www.researchgate.net/publication/339125514_Increased_Time_Outdoors_Is_Followed_by_Reversal_of_The_Long-term_Trend_to_Reduced_Visual_Acuity_in_Taiwan_Primary_School_Students