This post is by Phil Price, not Andrew.
I’m going to say right up front that I’m not going to give sources for everything I say here, or indeed for most of it. If you want to know where I get something, please do a web search. If you can’t find a source quickly, leave a comment and I’ll edit this post to provide one. For instance, I say below that many epidemiologists think a fairly substantial percentage of people with COVID-19 infections have no symptoms or only extremely mild symptoms, but I don’t provide a source. If you use your favorite search engine to search for, say [coronavirus asymptomatic] and you don’t see sources that agree with me, let me know. I agree it’s better to provide sources but I have work deadlines and I just don’t want to take the time. It’s bad practice but hey, this is just a blog.
Now, on to the topic of the post.
I hope we are all rooting for Sweden to find a way to limit coronavirus fatalities to a reasonable level while also maintaining their economy at a reasonable level. That would be a great thing for the Swedes, of course, but would also point a way forward for the rest of the world as we eventually try to let the economy get moving again. To me, the key distinction isn’t between voluntary restrictions on behavior (like Sweden’s) and requirements (like most of the rest of the world), but rather between whether non-essential interpersonal contact is or isn’t happening. If the Swedes are merely doing voluntarily what other countries are doing by law, the economic and social effects are going to be pretty much the same. But if they are implementing sufficient safety controls to limit the spread of the virus, and doing so in a way that permits most economic activity to continue, then we can do the same.
I do think it’s possible for a lot of business to proceed in an acceptable manner during the pandemic. I gave an example in a comment yesterday: the company that installed my HVAC system is still working, although doing many fewer jobs than usual, and they’re doing so in a way that I think is responsible. In normal times, they send a two-person crew to most jobs: a skilled HVAC professional and an assistant who schleps equipment and parts from the truck, wraps insulation, cuts metal, etc., under orders from the experienced person. But now they’re just sending one person to most jobs, even though it takes a lot longer and they now have an expensive person doing work that could be done by an inexpensive person. When they do have to send a pair of people, it’s two people who are only ever paired together, so if one of them gets sick they only put the other one at risk, they don’t rotate through the whole workforce. They ask the client to vacate the residence or at least the area of the residence where they’re working. They wear gloves and masks. Even thought they’re stretching and perhaps breaking the law on social distancing (here in the California Bay Area) by doing some nonessential work, it’s my informed judgment that what they are doing is OK.
So I can at least imagine a society in which companies shut down if they can’t provide a low-transmission work environment, but continue to work if they can do so safely, and in which people continue to see each other socially but do so in a responsible manner. I definitely, definitely would not trust the United States to be that society, at least not voluntarily, but maybe Sweden can manage it. Swedish politicians have said Sweden is special in that regard — more responsible to each other, more willing to follow government advice — and I can well believe that’s true, especially compared to the U.S. And if that’s the case, we in the U.S. can try to codify what works and make it happen here too.
Of course, there’s also the possibility that, even if Sweden is successful, that success simply can’t be replicated in the U.S. For instance, diabetes seems to increase the risk of death’ from the virus and I think we have a lot more diabetes here than in Sweden. Maybe true of other risk factors too.
And we know Swedes have been doing a lot voluntarily. According to the most recent Google Mobility Report (unfortunately from 9 days ago), person-hours at Swedish ‘retail and recreation’ sites were down 40%, transit stations about the same, and workplaces down 25%. Sweden has done a fairly substantial partial shutdown.
Is it enough?
Enough for what?
On the one hand some people say Sweden has pretty much won, they have the virus under reasonable control while maintaining a fairly healthy economy. On the other hand, they just moved into 10th place in deaths as a percentage of population, and seem on track to keep climbing the list: unless something changes they will soon take over 9th place from Switzerland, since Swiss deaths per million people only increased 40% in the past week, whereas Sweden’s doubled.
I’m going to set aside the economic question, because other than knowing Volvo is about to restart production in Sweden I know nearly nothing about Sweden’s current economic situation and I don’t have time to look into it. But I have been looking at the progress of the disease there, based on the sources I’m aware of, and…well, it’s a mixed bag.
As I mentioned in a previous post, Sweden’s death numbers show an odd pattern on Worldometers and the New York Times coronavirus stats page: they have a severe weekend undercount, which they correct later, but these sites only keep track of the latest totals, they don’t go back and adjust when they happened. That is, a coronavirus death is counted on the day it is reported rather than the day it occurred, and this seems to be a bigger issue for Sweden than for other countries. The effect happens on non-weekends too, it’s just smaller. Anyway it’s clear that on any day there is an undercount, which I suspect (not sure) may be a larger fraction in Sweden than in other countries.
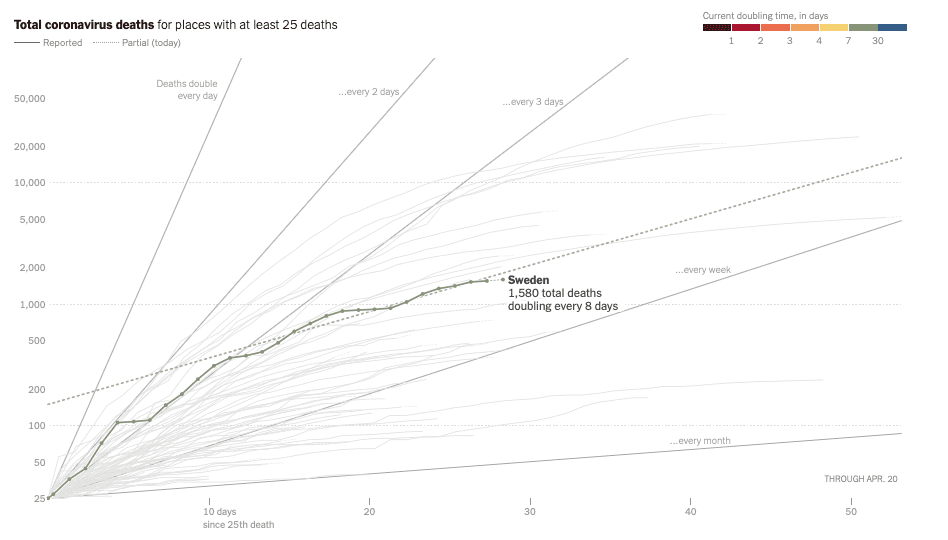
So, as of yesterday (Sunday April 19) they had at least 1580 coronavirus deaths, with deaths doubling every 8 days or so and no noticeable downward curvature on a log plot over the past two weeks. Most other countries that are at least a month past their first deaths seem to have slowed the increased the doubling time to more than 10 days, usually more than 12. And those doublings really multiply up over time: Four doublings in a month rather than three, that’s…well, that’s an additional factor of two in deaths, is what that is. Viewed through this lens, Sweden’s approach does not seem like a success. Yes, in deaths per capita they are still way under Belgium and Spain and Italy and the UK, but those are all countries that got started earlier and didn’t implement any kind of social distancing until it was too late to prevent mass casualties. Sweden, like the U.S., had time to learn from those other experiences.
So that’s the bad news.
The good news is, Sweden has not had the huge surge of cases (and subsequent deaths) that would have been expected if they weren’t taking effective measures at slowing the spread of the virus. Those voluntary measures they’re taking are definitely helping tremendously.
You know, even just writing this post has helped me put things in perspective. When I started writing I was baffled by what I saw as contradictions between claims coming from Sweden that they had been successful in controlling the virus while maintaining their economy, and the death numbers that seem to show no such thing, but now that I’ve looked at the numbers again and read a few opinion pieces again I am no longer baffled, I simply think there are different definitions of ‘success.’ Sweden avoided overwhelming their emergency health care system, as happened in Italy and Spain and New York. Maybe that’s what they mean by success. Yes, their per capita death count is still increasing faster than that of most of their peers, but not by a huge amount, and presumably they think they can bring the growth rate down soon. They might end up in the top eight or top five countries in deaths per capita — they’ll be number 9 in a few days — but that means there are several other countries that would be thrilled to be in their position just in terms of deaths per capita, and Sweden’s economy is presumably stronger too (I assume. As I said, I know nearly nothing about their economy). If avoiding the fate of Belgium and Spain and Italy is ‘success’ then Sweden is a success. To me that seems like an awfully low bar, but different people have different values and I’m sure lots of people would agree that that makes their approach a success.
Funny, by thinking about this post as I was writing it I have rendered it uninteresting to me. But what the hell, I’ll post it anyway, at this point the effort is all sunk cost.
This post is by Phil.
It sounds like whatever happened in Sweden (voluntary measures? luck or happenstance?) they’ve done what the USA media campaign claimed as the reason behind shutting things down. Maybe they are seriously fudging the reporting of deaths (more than ‘most anywhere else?) but another hypothesis would be that Sweden is simply a country where a crashed health-care system was unlikely to happen in the first place.
Just here in USA we have places which did roughly similar timing and intensity of shutdown to New York but which experienced something more like Sweden than New York in terms of “flattening the curve”. We even have places where less shutdown was done later (relative to New York) but the health care system was stressed only by the shutdown rather than a non-existent influx of COVID-19 cases.
So I’ll pitch my currently favored hypothesis. There are factors that cause a Lombardy or NYC level of health care system overload which are far more important than where on the spectrum of shutdown timing/intensity that region falls.
Under the counterfactual that New York City had moved two weeks earlier and somewhat more aggressively into shutdown than they actually did, I find it completely plausible that they might well have massively overwhelmed their inpatient/ICU/ventilator resources.
Under the counterfactual that some of the early-shutdown areas of California or Europe had waited another 2-3 weeks and been less thorough in shutting down, it is possible their health care systems might have survived without collapsing.
I think once real science starts being done to understand both the epidemiological and public policy aspects of this experience, it will be possible in retrospect to deduce other factors which trump the exact timing of a shutdown. And I am not talking about sticking heads in the sand and pretending their is no pandemic. I mean doing a Sweden type approach versus a San Francisco one as the possible range of responses worth studying.
The key to how high the infections go is how quickly social distancing was started relative to say the Nth community infection where N is a small fixed number. Let’s call it 20.
So, to tell us whether NYC vs say LA county were later or earlier, or more or less effective, and how much, you have to tell us the date they shutdown, the effectiveness of the shutdown, and the date they had 20 community infections (not ascertained cases, infections).
So, all anyone has to do is just figure out magically when the 20th community infection was… So it turns out that this is a really hard problem, and requires a fairly complicated bayesian model of the dynamics and of the testing, and of the effect of mitigation on the spread rate and soforth.
Without a detailed model that we can do inference from, the best guess we can do is say that if the early spread rate was similar in two places, then whoever got to a higher peak per day rate acted later.
So since NYC and LA had similar early spread rates in the cases, basically the evidence says LA acted earlier and that’s 100% why they have a dramatically lower peak than NYC.
Daniel,
I think the evidence is at best suggestive that the most important difference was timing of the shutdown. Making statements like “100% why…” in the absence of any reliable data on determinants, much less a well thought out model to incorporate that data, is just silly.
You have what we might call a “cognitive prior” that says “100% why…” by which I mean that’s what you believe and will continue to believe absent any overwhelming evidence otherwise. Given the paucity of evidence in this situation, if you want to stake out such an absolutist “prior” position there’s not much anyone can do to convince you out of it.
You seem to be pretty good at pushing back against every mathematical model that gives a conclusion that isn’t whatever your favorite conclusion is.
So far however you have had ZERO history of providing quantitative estimates of anything, except that you estimated a counterfactual that if we just reopened the economy we’d have about 20,000-50,000 more deaths and the whole epidemic would be over.
https://statmodeling.stat.columbia.edu/2020/04/18/the-evidence-and-tradeoffs-for-a-stay-at-home-pandemic-response-a-multidisciplinary-review-examining-the-medical-psychological-economic-and-political-impact-of-stay-at-home-implementation/#comment-1304891
So, please. Show us the calculations. I’d like to hear your model for what’s going on.
I don’t have a model and neither do you. You make up numbers that illustrate your own off-the-top-of-your-head guesses about the situation (which is usually something pretty dire). I make up numbers to illustrate my off-the-top-of-my-head guesses about the situation (usually something along the lines of “second worse respiratory virus EVER”).
The “calculations” you like to show are all Drake Equation type stuff where you multiply together a long string of guesses and assumptions and present the product as if it were somehow descriptive of reality. I’m not really interested in that sort of thing.
Here I try to spell it out: https://statmodeling.stat.columbia.edu/2020/04/20/coronavirus-in-sweden-whats-the-story/#comment-1310171
> that’s 100% why
The basic reproduction number is surely higher in NYC than in LA. Also, it seems that there were more independent introductions in NYC than in LA.
Sure, I can see that I should be more explicit. In reality, the growth rate in terms of per-day is irrelevant. All exponential growths at constant rate are equivalent when you express them in terms of a dimensionless time.
In the dimensionless analysis, all epidemic curves can be considered the same in the intermediate asymptotics between the early stages where the actual individual counts matter (ie. the new introductions, whether there were 30 or 31 cases etc), and the late stages when it stops being exponential. All we care about to understand the mitigation is this intermediate stage because all the action was in that intermediate stage. In the intermediate stage you can write:
Infections(t) = 20*exp(t)
where t is measured in e-folding times since the “apparent 20th case”. In other words t = (date – date0)/efoldingtime
t=0 is just the time such that as t grows in the region more than say 5, infections(t) approached the correct curve.
What it means to say that one place acted earlier than another then is just that their dimensionless time at the point where they took sufficient mitigation to dramatically alter the growth rate was at a smaller value for t.
that’s why it’s 100% t that matters, because as long as the growth was exponential with some rate, there’s a symmetry that makes everything else go away.
If you’re “lucky” in your region of the world, the efolding time is large so that you have many days to get to the same t and so can deliberate longer about the best plan. In both LA and NYC the efolding time was small, somewhere in the range of doubling every 2 to doubling every 4 days, which is efolding time of 3.6 to 5.8 days.
You said that “the best guess we can do is say that if the early spread rate was similar in two places“ but I think a better guess is that it was spreading faster in NY than in LA. You seem to argue that it’s irrelevant but I think we can agree that it’s easier to act “early” when that dimensionless time is flowing more slowly. The progression of the disease happens in standard time so when you observe 10 deaths or whatever it’s already “later” if the reproduction number is higher. It’s also easier to detect the first N locally transmitted cases and act “early” if those cases appear in a few clusters rather than several, by the way (you ignored that point).
Post-action the growth will no longer be exponential when the reproduction number is under control but those numbers will follow different paths in different places so the evolution of the system and the peaks will be different. You may want to reparametrize the time to force some symmetry but the progression of the disease and many other things relevant for the outcome happen in standard time and are not invariant under those reparametrizations.
> I think we can agree that it’s easier to act “early” when that dimensionless time is flowing more slowly.
Yes, I did actually explicitly say that, but the timescale was different between the two by the difference between 4 vs 6 days or something. Furthermore Wuhan and Italy gave us plenty of warning as to what would happen. In days, we had plenty of days to take action, yet we didn’t. This is why the news is full of exposes on what Trump knew and the news media keeps asking him why we did nothing in Feb.
>Post-action the growth will no longer be exponential when the reproduction number is under control but those numbers will follow different paths in different places so the evolution of the system and the peaks will be different
True, but the peak of cases in the hospitals etc occurs because of a backlog of cases that accrued in the exponential phase. We observe and hospitalize cases say 10 days after they’re created, which is ~ 2 dimensionless time steps.
To get a feel for the numbers, if dimensionless time is on the order of 5 days. Then there have only been 13.8 dimensionless time steps since Wuhan lockdown on Feb 11 and since there’s a ~10 day delay from infection to seeking care, and that’s 2 dimensionless time steps, we’ve had basically ~10 dimensionless time steps from the lockdown in wuhan to when the cases we’re seeing NOW were created.
LA cases per day started being constant April 1 or so. That’s when we saw the effect of Mar 19 shutdowns… so 13 days?
The big point is that once you knew an exponential growth was underway, you had *one* parameter to deal with: “how early in dimensionless time will you put in mitigation that drops the growth to subexponential?”
Anyone who knows anything about epidemics, and wasn’t playing political bullshit, would have and DID tell people: shut everything now.
This was hardly the first of its kind on Mar 10:
https://www.theatlantic.com/ideas/archive/2020/03/coronavirus-cancel-everything/607675/
if NYC had shut everything Mar 10, it would have been ~ (22-10)/5 dimensionless time steps earlier, and the hospital cases would have been basically 11 times smaller.
The hospital surge was entirely dependent on that one parameter: how many dimensionless timesteps did the region wait from the “nominal 20th case day” until they put in stay at home type orders?
I google it and see that it was Mar 22 in NYC and Mar 19 in CA. However local schools closed in CA on Mar 13, and other schools in CA were already closing first week of Mar. Many of the big employers were doing “work from home” first week of Mar. There were thousands of cases in Italy first week of March. We knew what was coming, and in that time period we had a unidimensional decision: what day to close everything. And it was always going to be worse the longer we waited. And all the articles arguing about how things worked in 1918 said the same thing… earlier was always better.
That’s EXACTLY what S Korea did, it’s what Taiwan did, it’s what Singapore did, they all got control as fast as possible in dimensionless time. And, because they devoted resources to test and trace, they also were able to get through their bolus of patients and do useful things earlier.
If you’re happy with your model that you explains 100% of the difference between NY and LA with a single parameter based on the point in the exponential phase where some non-specified mitigation action happens more power to you. This kind of universality reminds me of the IHME model that tries to fit all the curves into a common pattern but Italy has already failed to replicate the path of Wuhan. Italy is not Wuhan. NY is not LA. Adjusting one or two parameters may not be enough to account for the differences.
Carlos. Beyond the onset of mitigation of course the model is insufficient. But this model was sufficient for me on Mar 22 to make a public prediction (to my FB friends) that we would have the evidence to know for sure if we had flattened the curve in CA by April 12.
Which was in fact https://www.latimes.com/projects/california-coronavirus-cases-tracking-outbreak/
about 4 or 5 days past the peak of the 7 day moving average that LA times plots in terms of new cases. Now we are in more or less stasis with linear growth at 1200 a day for the last 10 days or so. I expect over the next 10 days further declines because it seems that CA is doing a pretty good job of at-home isolation but I have no magic crystal ball that extends outside the asymptotically valid intermediate range.
I freely admit there is no such symmetry trick I can do to simplify the problem down to picking a single number to predict how well we will do in the future. That requires actual epidemiology and knowledge of how well different policies will work. But during that phase, exponential growth unmitigated, all curves collapse to a single curve with the appropriate analysis.
Intermediate asymptotics are a super-valuable tool, anyone who wants to know more about them should read “Scaling” By G.I Barenblatt but the applicability is limited.
Today, we have a much harder problem. And we need leadership and epidemiological investigations. We need ways to measure, test, trace, track the stats, estimate whether growth is occurring, estimate prevalence, and of course figure out treatments and drugs and etc.
Do it. Model what you think happened. As I mess with mine I am seeing more and more that the number of actual cases had already peaked when the first US death was reported. Eg, the high variance in cases/deaths reported early on is only reproduced by the model if that is the case:
https://i.ibb.co/zsJ1L7t/apr20.png
https://i.ibb.co/RPxQYV6/sirresults.png
That isn’t a feature I expected to explain at all. Of course we can make the testing strategy more complicated to reproduce it too. As I keep improving it hopefully we can get a prediction out of it.
loool, ‘as I mess with mine’. That’s rich.
Daniel, I understand what you are saying. You model comparative infection growth by country using the date of the first N community infections (I’ve seen N = 10 used) as the starting point for tracking the hoped for S-shaped curve as the epidemic progresses day by day. AND you also do a per capita comparison of confirmed cases or fatalities, to adjust for different size populations for each country. Yet an earlier shutdown isn’t enough, certainly not an absolutist “100% why…”, LA had a dramatically lower peak than NYC.
I agree with Brent Hutto, that prompt measures for limiting virus spread and preventing healthcare system overload is important but by no means the only or even major determinant. This is epidemiology not just statistics. Unknown factors resulted in fewer confirmed cases, fewer deaths, and only mildly impacted healthcare systems in urban areas of Michigan, Georgia, and Louisiana than in New York City. Ambient temperature wasn’t the reason, because Michigan is cold unlike Georgia and Louisiana. Yet despite:
-much more poverty
-disproportionately adversely impacted populations
-imposing shutdowns later, and
-significantly less well-resourced medical facilities,
Detroit, New Orleans, and Atlanta have gotten control over and reduced numbers of COVID hospital patient admissions and deaths by 50% to 90% as of today.
Yes, California shut down before New York City, but its large urban areas such as San Francisco and Los Angeles are arguably more susceptible to a human to human transmitted disease (due to worse sanitary conditions, more homelessness, and the nation’s highest poverty levels) than New York City. There are additional confounding influences, such as the impact of New York City’s subway system, that can only be accommodated by an adequately detailed model. (There are no subways nor other public transportation in California.) This non-peer reviewed working paper The Subways Seeded the Massive Coronavirus Epidemic in New York City (JE Harris, MIT via NBER, 16 April 2020) is getting a lot interest. Other US cities have subway systems, but none as old and extensive as New York City.
Ellie:
According to this analysis by Alon Levy (“That MIT Study About the Subway Causing COVID Spread is Crap”, you shouldn’t blame the subway.
If subways aren’t a danger, then we need to rethink things. If crowding dozens of people together in close proximity is not a problem, then what *is* dangerous (besides a hospital full of sick people and extreme examples like that)? If subways are not a danger, then there must be a huge number of other things that are not a problem and we should identify them.
Or is the paper just bad, so: Paper = Bad .AND. Subway = Bad.
Living in Tokyo (with it’s massive dependence on (it’s amazing) public transportation system), I was convinced Tokyo was going to be an instant, incredible disaster. It hasn’t been. So far. New cases per day went up to 200 or so, and are now down to 100 or so (for the last two days) for a population of 13.7 million.
I went to jazz gig at a bar on March 19th, expecting the bar and trains to be empty on a Thursday. They weren’t. Coming home, the trains were crowded, the locals around me all quite inebriated. (Oops: Friday was a national holiday.) I thought I was going to die.
I’m still here. Go figure.
Four flaky theories. (1) Maybe masks really do help on the subways. (2) Maybe everyone really is washing their hands. (I am.) (3) The Japanese take their shoes off in their doorways, so they don’t track the virus inside. (4) Maybe the Japanese are just cleaner than Americans. (In my college days, I grew my hair long and shampooed it every morning, and a Japanese art history PhD candidate friend told me “You’re the cleanest non-Japanese I’ve ever met”.)
FWIW, the tube here this morning was discussing a cluster of cases from a karaoke party. Confined quarters, extended period, everyone breathing on the table, virus accumulating on said table, people touching said table, and touching their faces. One of the attendees had been in “close intimate contact with one infected person”.
To quote a friend who is a nurse at MGH: “We’re all going to die.”
Curiouser and curiouser. Every day, I know less about this thing.
It’s possible to agree that the MIT study is crap while still believing transmission risk is high in a crowded subway car. If you’ve got someone standing three feet from you, coughing coronavirus at you, that’s gotta be risky.
I wouldn’t think it would be controversial to say that the number of different people an infected person interacts with closely each day — ‘interact with’ meaning you spend at least twenty seconds within a few feet of them, or else you touch something they recently touched — is likely to be causally related to the risk of passing on the disease. If I were betting this is definitely the way I’d bet.
Of course, as others on this thread have pointed out, there are other factors too: what are household sizes, to what extent to old and young people share housing, what messages were people getting from politicians and other newsmakers, yada yada. But it’s hard for me to imagine the subway isn’t a factor.
Hello Andrew,
I just read it. I also read the 90 some comments, including one by the author of the NBER paper, physician Jeff Harris, who is a professor at MIT. Note that Alon Levy is a writer whose hobby and occupation is urbanism, having started his career studying math, according to the his bio.
Ad hominem aside, I will point out that Jeff Harris said (Disqus links don’t work well; try this http://disq.us/p/28p6keo or this https://nyc.streetsblog.org/2020/04/17/that-mit-study-about-the-subway-causing-covid-spread-is-crap/#comment-4879590864 for all of it)
Let’s see what other responses Harris has to Levy.
I’m just going to nod knowingly and pretend that I am following all this, while hoping someone figures all this out and comes back and tells us what is going on. Ellie, it sounds like you are volunteering to look into this further [he said nodding knowingly].
Yes, Terry. I volunteer. And I am here now to report my findings to you. Actually, I thought it would be clear after reading the quoted section but I truly did need to read the article that Andrew linked to first, to understand. I’m sorry about the ambiguity.
People who spend eight hours a day working in the New York City subway system are contracting COVID-19 at a three times higher rate than people who don’t. That’s why it might not be a good idea for the subway to remain open for the general public right now.
At the very least, it might make sense to shut the subway for a week like some New York City councilmen are asking Cuomo to do, in order to give it a deep cleaning. Reopen it after that and see if it helps.
Ellie:
I see, I see. That’s what *I* was thinking [he said nodding knowingly].
Ellie:
So is Harris right? Does his paper show this? To put it another way, is the Harris paper (A) crap, or (B) the opposite of crap?
Ellie, It does seem like many of the hot spots in the Levy article are where the NYC subway lines terminate. Which, assuming most essential employees enter these points to commute to the city interior? Yes, no, maybe?
Terry, Phil, Ellie:
Good points!
I warned about this on here like a month ago. It was obvious NYC was going to get hit hard like Italy and Iran due to that smiling robot: https://statmodeling.stat.columbia.edu/2020/03/07/coronavirus-age-specific-fatality-ratio-estimated-using-stan/#comment-1259326
Ellie: All those things you mention just change the time scale… You can ask “why is the time scale different from one place to another” but once you know that the growth is exponential… it’s all about “how many e-folding times have you waited”
So what *date* you put in your mitigation is not as important as *how many e-folding times did that date give your epidemic to grow*
Ellie, note that I’m not trying to minimize the role of Epidemiological investigations… WHY is the e-folding time different in different places in terms of physical aspects of the environment is very important in the long term to understand how to MANAGE the epidemic.
But in the early stages, the e-folding time in a given region isn’t under our control. it just is what it is and it depends on people’s mobility and the number of contacts per day and family sizes and school dynamics etc. In fact, I *define* early stages as the time past 20 or so cases and *until* we do mitigation that makes the e-folding time non-constant in time.
Before that point, our only control variable is *when* do we pull the trigger on starting the dramatic mitigation that changes the e-folding time.
“(There are no subways nor other public transportation in California.)”
You can tell that someone’s never been to San Francisco when they claim that BART (definitely a subway) and MUNI (mostly surface but underground and following the BART tunnels in downtown SF) don’t exist. CalTrain carries heavy traffic in and out of the city daily. And, of course, there’s an extensive bus system and limited trolley system. BART and MUNI alone carry close to 600,000 passengers per workday.
And San Francisco’s poverty level is lower than NY City’s, too.
Now, homelessness is a real problem …
Ha, I had missed that claim that there are no subways or other public transportation in California. That’s hilarious. WTF.
dhogaza and Phil,
Please no wtf at me. I lived and worked in Palo Alto for four years, got a graduate degree from Stanford. I took CalTrain many times, as well as BART and the trolleys and buses in San Francisco. There is still nothing comparable there to New York City’s subway. BART is below ground in places as are the trolleys, but not comparable to SF.
There is nothing in Los Angeles that even comes close to the New York subway system. Play nice.
Also, it is kind of irrelevant, because regardless of how little or much one likens the SF mass transit system to New York City’s, the fact remains that COVID-19 diagnoses and deaths are less than that of New York City by at least an order of magnitude. There is clearly something different going on between SF and NYC.
Oops, sorry typo:
>BART is below ground in places as are the trolleys, but not comparable to SF
should be
BART is below ground in places as are the trolleys, but not neither are comparable to the underground transit system in New York City.
Aren’t you forgetting some of the, in my opinion, biggest differences between LA and NYC:
1. LA is spread out over a wider area meaning you meet fewer people on a normal day in LA than NYC
2. More people use public transport in NYC than LA and The NYC commuters come from a wider socioeconomical background
This results in average newyorkers comming into contact with more people and those people are from a wider background.
> So I’ll pitch my currently favored hypothesis. There are factors that cause a Lombardy or NYC level of health care system overload which are far more important than where on the spectrum of shutdown timing/intensity that region falls.
> Under the counterfactual that New York City had moved two weeks earlier and somewhat more aggressively
> Under the counterfactual that some of the early-shutdown areas of California or Europe had waited another 2-3 weeks and been less thorough
Why are these counterfactuals the ones to think about if the question is to try to think about factors other than shutdown timing/intensity on healthcare system outcomes?
My points being two:
1) There may be some places (perhaps NYC) where it literally was not possible act soon enough to avoid an overwhelmed hospital system
2) There may on the other hand be places where no matter how much “too late” they shut down, the hospital system would not have been overwhelmed.
I’m saying depending on some as yet unknown/unstudied important, major factors the ability of “social distancing” policy to determine the course of events may be insufficient to change the outcome.
Hey, thanks, Phil Dude!
Not sure what you’re thanking me for, but you’re welcome!
> Those voluntary measures they’re taking are definitely helping tremendously.
I guess the obligatory measures (like gatherings of more than 50 people being banned and bars being table service only) have contributed as well.
Discussion on these blog comments seems to continually feature an expressed or implied attitude that someone, somewhere is arguing in favor of doing absolutely not one blessed thing in response to a major public health emergency. As far as I can tell that is a strawman. As I mentioned in my comment above, surely at this point the range of possible policy options we need to discuss does not include ignoring the virus altogether and packing 50,000 people into soccer stadiums or anything of that ilk.
From what I’ve read, Sweden was fairly timely in making mandatory the obvious measures that nobody in his right mind would argue against. The difference in “The Swedish Experiment” is stopping there and making everything else suggested, optional or voluntary.
It’s kind of odd (to me at least) that a society often thought of as the stereotypical social democracy has more faith in the judgement of its individual citizens than places which like to style themselves exemplars of robust individualism.
Believe it or not, some people are opposed to the closing of nightclubs and the cancellation of parties, concerts, sports events, religious gatherings and whatnot. Anyway, I was just pointing out that there were also restrictions imposed by law in Sweden. That’s all.
Carlos, sorry. I guess I shouldn’t have said “nobody” was proposing that stuff. I keep losing track of the world we actually live in, full as it is of numbskulls and arrested development cases. Sigh.
> Discussion on these blog comments seems to continually feature an expressed or implied attitude that someone, somewhere is arguing in favor of doing absolutely not one blessed thing in response to a major public health emergency. As far as I can tell that is a strawman.
Then you are not looking very hard.
Effectively in the case of Sweden we have a temporal autocorrelation issue, leading to a much smaller effective sample size if we were trying to estimate their pandemic curve.
Also I recommend articles on how good Sweden is be written on Wednesdays, not Mondays.
> Wednesdays, not Mondays.
This is true but almost funny.
Its hard for people not to see rainbows when they are in dire situations (e.g. early reports of effective treatments and recently a biased analysis that suggest ACE markedly decreases mortality. Never digest science before it has been adequately aged).
The Swedish death rates are updated daily by the Swedish Department of Public Health (Folkhälsomyndigheten) with the actual dates of death. The dates are not corrected in the Johns Hopkins or Worldometer or wherever they track daily deaths, only at the department’s website. It makes quite a difference to the curve, since most reported deaths happened many days or even weeks earlier. We are now seeing a plateau.
You can check it out at https://experience.arcgis.com/experience/09f821667ce64bf7be6f9f87457ed9aa
I don’t know if there’s an English version but if you’re looking for deaths, the word in Swedish is “Avlidna”. “Åldersgrupp” means “age group” and “dag” means “day”.
How deaths are reported is also important. What systems are being used? How is it organized? What is being fed into that system? Is that same system used by everybody? Someone called Sweden a “statistical powerhouse” in an article and that is an apt description. In the this case, the Swedish personal ID number is an important factor. Every Swede is given a personal ID number at birth (or at permanent residence) and that number is used in every interaction with institutions like health care, banks, libraries, for employment, memberships in organizations, everything. All reporting is centralized, the same systems used by all entities private or public. This means Sweden can know and verify deaths faster and more accurately than probably any other country. (If you can find a country that’s actually faster I’d like to know how that is organized) It is impossible to get “lost” in Sweden. You will not find bodies hidden and stacked in nursing homes like what has happened in Spain and the US. This also makes a difference. The weekend lag is real, but all other countries and states also lag – and not by a day or two. Why the weekend lag is more pronounced in Sweden is probably related to this.
Thanks, it is hard to know what are real differences and what are artifacts.
In Canada we have had 1,758 compared to Sweden’s 1,765, but we have almost 4 times Sweden’s population. With universal heath care, a health care system currently with some extra ICU space and most of our deaths in nursing homes, I don’t believe there is that long of a delay in reporting deaths…
And of course, differences in demographics – Demographic science aids in understanding the spread and fatality rates of COVID-19 https://www.pnas.org/content/early/2020/04/15/2004911117#sec-1
Looking at Worldometer.
I was comparing identified cases per million to numbers of tests per million. Obviously, those two metrics should be viewed in relationship to each other. Sweden ranks lower, relative to other countries like Switzerland, in the ratio of number of tests to identified cases. That’s not a particularly good sign.
Sweden only does strategic testing. Which means they only test people who need hospital care and health care workers showing symptoms. They test only when a positive test would change something. If you have symptoms but you don’t work in health care and you don’t need hospital care, the rule is you stay home and isolate. A test would then change nothing. A negative result could even be detrimental, as it could give a false sense of security, when you could get infected the next day.
Instead, Sweden does random testing particularly in Stockholm (where the outbreak is) to get an idea of how many are infected at a certain time.
If there was an infinite test capacity, maybe you could choose a different strategy, but I think having some system is necessary.
Ani –
Thanks for the information.
> They test only when a positive test would change something. If you have symptoms but you don’t work in health care and you don’t need hospital care, the rule is you stay home and isolate.
FWIW, I would guess that “compliance” with such a directive, and the ability of people to follow such a directive (given the levels of social support) in Sweden is higher than in the US.
> Instead, Sweden does random testing particularly in Stockholm (where the outbreak is) to get an idea of how many are infected at a certain time.
Yah. That seems to me like a very good metric for assessing the degree to which a government should mandate social distancing – but it doesn’t have to happen mutually exclusive with testing people with symptoms.
> If there was an infinite test capacity, maybe you could choose a different strategy, but I think having some system is necessary.
Something must be up with my keyboard as posts keep going up before I’ve hit the “submit” key…
…
Anyway:
> If there was an infinite test capacity, maybe you could choose a different strategy, but I think having some system is necessary.
I completely agree. But the underlying question there is why isn’t our capacity greater. IMO, increasing capacity should be a priority. Another question is whether some complacency can develop to the extent that people start of focus resources and energy on a policy of limited testing.
Please beware of drawing conclusions about miltivariant causality by comparing a singular variable.
Sweden is vastly different from the US, and in particular certain parts of the US, along a long list of attributes. Yes, like prevalence of diabetes, but also issues like population density, number of average people living in a household, access to healthcare, etc. They even differ greatly along important metrics from more similar countries like Switzerland, such as in proximiy and degree of travel to/from an “epi-center” like Lombardy.
I think it makes little sense to compare the impact of social distancing policies across countries unless you do a whole lot of work to control for potentially explanatory variables. Especially when the quality of data, at least at this point, are so poorly validated, so variable across context, so quickly evolving, so much just a singular point in time, More than likely, such exercises based on cross-sectional data, without the power of longitudinal analysis, serve better to confirm biases than anything else.
Multivariate…
That’s why my default position is, show me what really determines where the health care system is going to crash and where it is not. How do you distinguish New York City and Detroit from Stockholm and Dallas? Then once we understand that we’re ready to ask questions about social distancing.
Sorry to intrude this beatuful discussion but can’t constrain myself. Apropriate term is acually phisical distancing.
That’s as may be but I have yet to hear the phrase “physical distancing” uttered even once while the phrase “social distance” has occurred in (my rough estimate) 99% of conversations I’ve had with anyone over the past month.
‘Social distancing’ is an oxymoron, just like ‘alone together’.
How is distance sociable?
Actually, in terms of proximity to the Lombardy epicenter, the Stockholm outbreak (which has more than 75% of cases and deaths in Sweden) started when thousands of people came home from spring break skiing in Italy late February. They tried testing and tracking all of them and did fairly well, but testing capacity was low at that time and community spread was soon a reality. Mitigation strategies were then implemented, social distancing, closing of universities, working from home etc. Intensive care capacity was more than doubled and so far 20% of icu beds have not been used.
The plurality of deaths in Sweden are people 80 years and older, many 90 years and older, who got the virus in nursing homes and died there. Most seniors in Sweden receive help, care and service in their own homes and do not move into nursing homes until they are very sick and fragile, so fragile that on on average they die within months of moving into one of these homes. Those homes are like little live-in hospitals, and if the virus gets into a place like that, a lot of people can get infected before it’s discovered. Social distancing, voluntary or not, is not possible since they require 24/7 care from nursing staff coming and going in shifts.
These seniors are too fragile to endure or survive intensive care (intubation, for example, is likely to cause only suffering with little result). They are thus are given care by the doctors and nurses at the nursing home and are only moved to intensive care units if the physician think the patient would have a chance of surviving it. Sweden is now rethinking not their mitigation strategy as a whole, but the nursing homes – their size, the way they are staffed, how the rules and incentives for privately run nursing homes are working. The coronavirus has exposed some serious flaws in the capacity of the current system to protect the most vulnerable elderly and this is what is being discussed in Sweden today. Not the mitigation strategy, which has broad popular support and is followed by most people, most of the time.
It’s hard to know how many of those seniors would have died within the next few months anyway, but Sweden is tracking the overall mortality and comparing it to the average of previous years.
Thanks for the info.
Thanks, Ani.
I wish all-cause mortality numbers were easier to find and were more frequently updated. I would be as interested in those as I am in deaths attributed to COVID-19.
Old people everywhere are way more vulnerable to the virus. About 15% of Sweden’s reported coronavirus deaths are under 70, and 5% are under age 50, I think those are not atypical of other countries. I also wish data on life-years lost were routinely available, rather than just ‘deaths’, but I haven’t seen a compilation of such data.
I recently read an article that quoted Swedish nursing home attendants who were dismayed and angry about the lack of support they’ve been getting. No protective gear, no disinfectant. One of them said they know there are asymptomatic people, they know some of the nursing home staff must have the virus and must be infecting the residents, but they are given no way to protect them. (I was going to mention this in the post, but forgot). This seems odd because the resources that would have to be made available are so small.
My worry about Sweden is similar to my worry about California (where we did a relatively early shutdown): the number of deaths so far is relatively low and we are nowhere near exhausting the capacity of our hospitals, but the number of deaths has been growing exponentially for the past two weeks with a roughly constant exponent. The growth rate is similar to Sweden’s, a doubling every 8 days or so. Sure, it’s not the doubling-every-3-days that we’ve seen in some other places, but still, if we don’t bend this curve further at some point then things will eventually get bad. Those remaining 30% of hospital beds can fill up in a hurry. (And of course, to the people who are dying and their families it is already bad). The lack of further progress, day after day, is disturbing. I’m aware that deaths is a lagging indicator of infections, and in both California and Sweden there’s reason to believe or at least to hope that infections are slowing, but neither place has done sufficient testing to be sure. It just seems way too early for a victory lap. When there’s a week with fewer deaths than the previous week, that’s when I’ll breathe a sigh of relief.
Absent an effective vaccine and/or widespread screening, testing, tracing and segregation of newly infected persons just about everyone is going to eventually be infected with this virus. And a large proportion of the oldest and most vulnerable people who get it are going to die.
So starting early or being more hardcore with the shutdown is literally to spread out the inevitable. Not to avoid the inexorable spread of the virus throughout the population. That will only happen through immunity (herd or vaccine) or an extremely difficult and expensive to implement classical Public Health approach.
P.S. I say “extremely difficult and expensive to implement” because of COVID-19’s particular combination of ease of transmission, largely asymptomatic presentation and long period of shedding virus. It makes half-measures of testing and tracing nearly useless IMO.
I have my doubts about a vaccine since there has never been a safe and effective coronavirus vaccine. But why do you assume a large proportion of the most vulnerable need to die? Most of the deaths seem to be due to aggressive use of high pressure ventillation which is dropping out of favor and hyperbaric oxygen therapy is reported to improve all the strange symptoms. Combine that with fixing the vitamin c deficiency that undoubtedly exists (I guess this hasn’t been measured because people are worried about contaminating the HPLC machines) and you can easily reduce mortality by 10-100x.
Also, spreading out the inevitable may be worse than you think. If antibodies wane after a year or so in the 80-90% of mild cases (like for some other coronaviruses) flattening the curve pretty much guarantees the virus becomes endemic vs burning itself out.
Given what little I know about vaccine efforts for other coronaviruses, plus the history of influenza vaccines, I would be very surprised if a highly effective COVID-19 vaccine will be available any time in the next year or two. Never is a long time and something may eventually be found but it is highly unlikely to come in a meaningful time frame for dealing with the ongoing spread of the virus.
I sincerely and devoutly hope to be proved wrong on that.
And it very well could be that a few puffs on a cigarette fix the loss of spontaneous (non-intentional) breathing like reported for mountain climbers and the Tour de France cyclists when they climbed into the alps.
But we know that it’s better if everyone dies and western civilization is destroyed than to ever recommend that treatment.
New smoking data out of France: https://www.qeios.com/read/article/574
Phil, CA has not been growing exponentially. New cases are growing linearly at a constant ~1200 per day for the last ~20 days.
https://www.latimes.com/projects/california-coronavirus-cases-tracking-outbreak/
Sweden on the other hand is still in exponential phase as far as I can tell so far
https://ourworldindata.org/grapher/daily-cases-covid-19?time=..&country=SWE
But they are much earlier in the curve, at only 500 per day and they are doubling every ~ 8 days. If they continue like that they will be at CA levels next week, and at NY levels of 10000 cases per day in log(10000/500)/log(2)*8 = 34 days
So again it all comes down to when they will get out of exponential phase… People don’t seem to get exponential growth. It eats everything. If you are in exponential growth with COVID you have ONE goal… End the exponential growth . That’s it.
Sweden will end the exponential growth, the question is just how costly will their math lesson be.
Sweden had the highest reported cases per day 2 weeks ago according to that. Doesnt look like exponential growth to me.
Hmm… strange that this morning when I pulled up that graph it looked VERY different from the way it does several hours later… :-(
Not sure if maybe I got some kind of cached version, or something else… but I agree with you now that they’ve been flat with a lot of wiggles for ~ 2 weeks.
Perhaps I’m overly skeptical of looking at ‘cases’. A few weeks ago it was pretty useless: it was very context-sensitive, and in places like New York and northern Italy that were overwhelmed by hospital patients and underequipped for testing it was clear that lots of serious infections were not recorded as cases; at the same time, from all-cause mortality it was clear that this was also true in many other countries too, even those that weren’t overwhelmed. So I’ve only been looking at deaths, well aware that they lag infections by a month or so. Sweden and California are both growing exponentially in deaths.
But for countries that aren’t overwhelmed, cases are clearly informative, especially once we are out of the phase of rapid growth. And yeah, Sweden and California have both leveled off, so deaths per day should start dropping soon and the cumulative death plots should flatten. I’m still not going to breathe easy until I see that happen — just worried about various ways infections can fail to convert to cases but still lead to death — but I agree it looks like it’s coming soon.
Daniel –
Isn’t it critical to consider the ratio of tests conducted to cases identified before trying to infer future growth?
Sure, but Sweden seems to have started testing earlier than the US and grown quite quickly though not quite as fast as the US, so I don’t think they’ve saturated their testing capacity.
swedish vs us testing
Thanks for the link. I’ll check it out.
I was looking at Worldometer, and just eyeballing, it looked like their ratio of tests per million to cases per million was relatively low compared to other countries with high cases per million rates.
This is great contextual info. Thanks much!
BTW, I’d still guess a lot more travel between Lombardy and other countries in Western Europe than to Sweden. One of the reasons I’m skeptical of cross country comparisons to evaluate policy effectiveness without better data and a lot of control of potentially explanatory variables.
The pull to see patterns and draw conclusions about causality is very strong. The antidote to that I a better data and control.
Definitely Switzerland is more connected to Lombardy than Sweden. Over 65’000 people cross(ed) the border daily to work in the Italian-speaking canton of Ticino. Population 350’000, 2900 cases and 270 deaths. It may make more sense to compare Sweden to other Nordic countries than to Switzerland.
Well, it depends on whether you account for the differences between the Nordic countries and the regions therein. And just chance and random distribution. The outbreak in Sweden is happening in Stockholm, and other regions of Sweden have seen very little of Covid in comparison. Stockholm is with 1.3 million inhabitants (2.4 m metro) the most populated Nordic city (it calls itself the capital of Scandinavia). Swedish schools have a winter/spring break especially meant for doing winter sports (it’s called “sport break”) in February, but different regions have their break different weeks due to different climates. Stockholm had its winter sport holiday late February, so thousands of people travelled from Stockholm to Italy and the alps. Schools in other Nordic countries do not have this particular tradition.
So odds of Scandinavia seeing the first large outbreak in Stockholm were pretty low.
Also, I think it’s a mistake to count deaths or cases per capita this early. And it is still very, very early with this virus. Thing is, an outbreak grows in absolute numbers, with each one person spreading the contagion to X others. It also has a kind of speed, set by parameters such as when and how long the virus is contagious and it’s incubation period. It does not care how borders are drawn. Someone used the analogy of a forest fire, it does not matter how big the forest is or what different parts of the forest are named. It burns until it runs out of trees. It just takes a longer time to burn 25% of a largely defined area compared to a smaller one. And the absolute number of burned down trees could be the same.
Can you imagine how absurdly, impossibly fast the virus would have had to spread in the US to infect the same percentage of US 327 million people in the same time frame as it infected 10 million Swedes? Maybe comparing outbreak to outbreak would be more useful. But then you’d still have to account for density, demographics, climate, holidays, infrastructure…
I’m not sure any useful comparisons between countries can be done at this point.
And you can slow the virus down, but no one thinks you can eradicate it. It will take years before a vaccine is not only developed, but distributed. If we even get there at all.
“Can you imagine how absurdly, impossibly fast the virus would have had to spread in the US to infect the same percentage of US 327 million people in the same time frame as it infected 10 million Swedes?”
That’s just 5 doublings. With 3 days per doubling, it’s sufficient for the virus to have reached the US two weeks before it reached Sweden. Exponential growth is funny that way.
Consider an old riddle: imagine a pond with water lilies. The water lilies grow unchecked, there was one lily on the 1st day, 2 lilies on the 2nd day, 4 lilies on the 3rd day, 8 lilies on the 4th day, etc. The pond is completely covered with lilies on the 18th day. When was the pond half covered?
Mendel –
> Consider an old riddle: imagine a pond with water lilies. The water lilies grow unchecked, there was one lily on the 1st day, 2 lilies on the 2nd day, 4 lilies on the 3rd day, 8 lilies on the 4th day, etc. The pond is completely covered with lilies on the 18th day. When was the pond half covered?
Thanks. What a great way to get people to think about exponential growth.
Ani-
Thanks for that information.
Although I’m skeptical that in the end the same % of a given population will get infected irrespective of interventions, I will point out that there may be any variety of advantages to slowing the rate of spread, including the potential of reducing fatality rates from the development of therapeutics and preventing hospitals and healthcare workers from getting overwhelmed snd/or exhausting resources
I don’t think any of that suggests that Sweden is more comparable to Switzerland than to other Nordic countries.
And, from the Wikipedia numbers at least, Stockholm doesn’t seem so different from Copenhagen. The population of the urban area is 22% higher (1.6mn vs 1.3mn) but it’s also less dense (4200 vs 4500 per km2). For the metro area the population is 15% higher but with a much lower density (2.4mn, 360 per km2 vs 2.1mn, 1200 per km2).
I can’t find how many cases happened in the Copenhagen but on March 11 when the Danish government announced the closure of schools and other measures, there were 516 cases reported in the country. They were 620 in Sweden, including 266 in Stockholm county. Per 100’000 there were 9 cases in Denmark, 6 in Sweden, 11 in Stockholm county.
It also seems unfair to say that the outbreak is happening in Stockholm only, every county has now more cases reported per capita than Stockholm had one month ago.
Indeed. If you want a solid couple for a comparison, take Finland vs. Sweden. The former has followed the de facto standard restrictive approach, while the latter has followed its unique path. But both societies are pretty much similar in all relevant dimensions.
But we neeed to wait a year to see what the deaths are – Finland haven’t changed the 0.2% CFR, just the dates.
Agreed. In such decision making in face of so much uncertainty, it seems to me that a guiding principle should be to hedge against the largest categories of downside risk, even low probability high damage function risk. Of course, there there is huge downside risk to shutting down the economy.
It’s not hard to get an idea of how things are going in a country as a whole if you look at the fractional rate of change of new cases per day. This relates directly to the R0 number, the number of new cases one infected person causes. Yes, maybe there are ten or 20 unknown cases for every one confirmed, but as long as we can be consistent in using confirmed cases, we can use the published data.
Here’s how the basic calculation goes. The actual number will presumably vary from country to country, if you have a way to discover what the underlying number are. A value of R0 > 1.0 means exponential increase in the case count, a number less than 1.0 means the new cases are dwindling. We’d hope to see a number much less than 1.
Suppose R0 = 3. We often read that it’s in the range 2.5 – 3. And let’s take the period during which a person can pass on the disease is 10 days. Yes, we hear 14 days, but that’s an outside range. You have about 5 days where they don’t have symptoms and another 5 days during which they are clearly sick. If they get very sick, either they go to the hospital or other people are more careful around them. So about ten days.
Therefore an infected person will infect about 3 / 10 = 0.3 people /day. That is a fractional infection rate of 30%/day. In the US after the initial pulse of infections, that’s just about the number we had for several weeks. If continued, a 30% growth rate would lead to a frightening number of cases.
An R0 of 1.0 would mean that the growth curve has “flattened” – that it is no longer growing. For a nuclear reactor, it would be the regime of constant power. The fractional daily rate for this condition would be 0.3 / 3 = 0.1, or 10%/day growth rate. If you look at the data for the US, sure enough, the daily growth curve becomes just about flat at about the 0.1 value.
So for the US data, at any rate, assigning an initial R0 value of 3 seems fairly close to the mark. I’ve seen the same thing for many other countries, too, but not all of them. The current value for the US is around 0.035, or 3.5% / day. That difference would be what social distancing, closing down parts of the economy, and the other things we’ve been doing have achieved.
These data are taken from the John Hopkins time series data, BTW.
If you look at the data for Sweden, there is some weird behavior in the confirmed case count – now apparently taken care of -, but the death counts look normal (i.e., like many other countries) except for those large ups and downs that others mentioned in earlier comments. In particular, the fractional daily growth rates track the U.S curve very well (except for the ups and downs) except for one thing.
After the Swedes experienced an initial surge in deaths, their response as shown by the fractional daily deaths started dropping nearly two weeks sooner than in the US relative to its initial pulse (the big pulse came about earlier in the US than in Sweden).
Hi there, just two pieces of information that are important to consider when evaluating Sweden. Important to remember is that countries count COVID deaths in different ways, which makes the figures very seldom easily comparable. In contrast to most countries (e.g., the Netherlands, the UK, and Norway), Sweden (just like Belgium) includes deaths at nursing homes, at home, etc., and not just “hospital deaths” (which is the case for many other countries). That makes a very large difference for the numbers (around 1/3 of totals). In addition, and perhaps even more important, the Swedish count is of “deaths with COVID” (someone died, and had the virus), it is not a count of “deaths of COVID” (someone died, had the virus, and the cause of death was deemed to have been the virus). The issue of how many who died because of COVID instead of just being infected by COVID, will be sorted out later. Thus, had other countries counted their COVID deaths in the Swedish way, Sweden’s figures would have looked much less serious when compared to other countries. Unfortunately, these Swedish counting principles are almost never mentioned in news articles about COVID in Sweden. Note, what Sweden still has many unfilled ICU beds, and the healthcare system (while strained in some areas) is overall not strained: the system I coping.
Birger, thanks, this is a good point, and one that I know the Swedish health authorities have emphasized. But Sweden is not alone in this definition; for instance ” In Italy, any death in a patient with positive reverse transcriptase–polymerase chain reaction (RT-PCR) testing for SARS-CoV-2 is considered COVID-19 related”; and for the past week the U.S. has been counting both probably and confirmed COVID-19 deaths as defined by this standard: “A confirmed case or death is defined by meeting confirmatory laboratory evidence for COVID-19. A probable case or death is defined by i) meeting clinical criteria AND epidemiologic evidence with no confirmatory laboratory testing performed for COVID-19; or ii) meeting presumptive laboratory evidence AND either clinical criteria OR epidemiologic evidence; or iii) meeting vital records criteria with no confirmatory laboratory testing performed for COVID19.” Several other countries have either always used, or have switched to using, criteria not very different from Sweden’s. Maybe most have, I don’t know. Anyway I think this is a good point to keep in mind but I don’t think it changes the overall picture much, at least with numbers from recent days.
https://www.nytimes.com/interactive/2020/04/21/world/coronavirus-missing-deaths.html
To be fair it does seem like Sweden is doing a better job of accounting for its Covid-19 deaths. At least by looking at all-cause mortality Sweden does not have a large number of unexplained excess deaths sofar.
Nice post Phil, thanks for going to all the effort.
I can kinda see why you lost interest in it: the mystery revealed banality. Sweden is using a novel approach to have roughly the same disaster, at least in terms of lives lost.
But IMO it’s better than you make it out to be, since they won’t have to repay the borrowing. Very *very* roughly the US has borrowed $3Trillion, which works out to roughly $10K per person. That’ll take some healthcare out of your future.
Phil:
Good job. Nice to have some level-headed overall assessment. Things have gotten way too complicated to try to do this by oneself.
Phil:
Sweden has a substantial immigrant population. Does that factor in any way? I’ve heard immigrant areas have been particularly hard hit. The most hard-hit European countries also look to have substantial immigrant populations.
Hi, As a Swede, I can confirm that Syrians and Somalis are highly overrepresented among the “deaths with Corona”, due to highly localized disease spread in some areas in Stockholm, but their proportion of the totals is still small. While 50% of Swedish households are composed of singles (social distancing by default), the opposite is true for Somalis and Syrians, where families (writ large) can be very extensive, large and close (no social distancing by default). At the aggregate, the “deaths with COVID” (not to be confused with “deaths of COVID”) are almost exclusively in the age span >70 years old.
The group who fall under the heading “immigrant” in a country like Sweden live in the same socioeconomic niche as non-privileged minority groups in USA or any other wealthy country. As such, I would be willing to bet they will be battered by this much more badly than the middle-class and wealthy. It’s virtually axiomatic that in any society economic or health problems fall heaviest on those at the bottom of the socioeconomic pecking order.
+1
Actually I haven’t seen too much data on ethnicity or immigration status, the thing that stands out to me is that 90% of fatalities are over the age of 60, and a majority of those are over age 80, so I’m not sure how that jives with immigration status or ethnicity, but my guess is that the affected nursing home population is overwhelmingly native (e.g., European in Europe, American in the US).
Also relevant: what percentage of the staff of nursing homes consists of immigrant?
> Yes, their per capita death count is still increasing faster than that of most of their peers, but not by a huge amount, and presumably they think they can bring the growth rate down soon
> They might end up in the top eight or top five countries in deaths per capita — they’ll be number 9 in a few days
Eeeh, I’m not super convinced by the line fits. At least if we’re going by the stuff plotted it doesn’t seem obvious to me that they’ll move up the ranks (though it doesn’t look like they’ll move down either). I could easily be reading it wrong though.
The plot shows deaths, not deaths per capita. Switzerland’s deaths per capita is increasing 45% per 8 days, Sweden is increasing 100% per 8 days, and deaths per million is 165 (Switzerland) versus 155 (Sweden). Multiply the first number by 1.45 and the second by 2 and you have an estimate of where they’ll be next week. That’s not a guarantee, of course — Sweden could start to flatten out tomorrow, or maybe already has (hard to know, given the large ‘weekend effect’ in the counts, which takes days to resolve) — but if I were to bet on something so macabre I’d be betting for Sweden to overtake Switzerland.
I found this chart helpful in thinking about the Swedish reporting delay.
The gray bars are a simple constant approximation to the number of lagged reports with a given delay, if I understood the R code right. Based on that model, Sweden is also past the (first) peak.
https://adamaltmejd.se/covid/
Very helpful indeed, thanks!
Phil:
A lot of discussion assumes a one-size-fits-all thinking. But there is a h**k of a lot of heterogeneity. Is it possible to accomplish a lot by focusing more narrowly? For instance, banning groups of more than 10 or 5 seems like it would accomplish a lot. And making people stay 6 feet apart would also accomplish a lot more. Also, there seems to be little transmission by touch. Also, supers-spreaders seem to be a very big part of this.
My question is, would it be possible to accomplish a large amount with very narrowly focused prohibitions?
I didn’t say this very well. Let me try the inverse.
Are there things we can just ignore (rather than be super careful about everything) because the risk is so low? Can we just forget about gloves and touching things? Can two-person HVAC teams forget about masks (just stay away from the customer)? Can we not worry about hanging out with good friends if no one seems to be sick? Can we play non-contact outdoor sports without worrying about anything? Can we eat takeout food without any precautions?
All good questions, Terry, by which I mean I don’t know the answers…although I did read an article by a doctor that says transmission from food is unlikely, and hey, if a doctor says it it must be true.
It’s obvious that activities aren’t either ‘safe’ or ‘risky’, there’s a continuum; also the risk doesn’t just depend on the activity in a generic sense (even conditional on an infected person being involved) but on the details of how the activity is performed. But how to determine which ones are most risky, and here to draw the line between what is and isn’t acceptable..your guess is as good as mine, or quite possibly better.
+1 to second paragraph
To Phil the blog post author,
I have a minor disagreement with one of your behavioral assumptions. You describe the virus response measures taken by a company who services HVAC in California. It seems responsible and well-reasoned, as a way to mitigate risk. It is my informed judgement that their changes to business operations, to minimize the chances of virus infection, will be effective, which was your conclusion as well. Next, you say,
Phil, why would you not trust companies in the United States to make the decision to shut down if low-transmission work is impossible? You just gave an example of an exemplary American HVAC company who took all sorts of measures, voluntarily, to ensure a safe environment for workers. California is part of the United States.
The latter part of the passage you quoted sounds like uh Swedish exceptionalism to me. No, that’s an overstatement. Yet it is naive to readily accept the word of Swedish politicians who claim that Swedes have superior morality compared to other nations. And then you extrapolate to the US, that such upstanding and ethical behavior is inconceivable.
Andrew wrote a post about avoiding political bias in analyzing the COVID-19 pandemic and an effective response. The United States is not a failed state, without rule of law, and utterly lacking in business ethics. If that were the case, our financial markets wouldn’t be the most liquid, deep, efficient, and transparent in the world. Be careful of preconceived biases.
Thank you for the link to world rankings of per capita-adjusted COVID-19 deaths by nation. I was glad to note that the United States is in position #12 with the following more ethical, responsible, trustworthy nations (well, some of them, e.g. Sweden) having higher death rates in ascending order of lethality: Ireland, Sweden, Switzerland, Netherlands, UK, France, Italy, Spain, Andorra, San Marion, and Belgium. We’re not doing so bad, despite all the blame heaped on Dr. Fauci and Donald Trump and Dr. Birx and the CDC.
Ellie,
Standing ten feet from each other, the owner of the HVAC company and I had a long conversation in which we discussed the coronavirus response and how his company is handling it. He said he has had trouble getting some of his employees to take the rules sufficiently seriously, but he admitted that he might have felt the same way except that his wife is a nurse so he (1) is worried about her, and (2) hears her stories about what the patients are going through. He also said that after the Bay Area counties had issued shutdown orders, but before California had done so, one of his employees went to Tahoe to spend the weekend snowboarding with friends at a ski resort. Actually they only did it on Saturday, since the ski places were all shut down the next day. But the point is that unless the place was shut down, they were doing it. One of my wife’s friends did the same thing on the same weekend, going to a shared ski house (5 couples) for the weekend, but having it shut down after one day.
And of course there are all those mayors and governors who tweeted messages encouraging people to go about business as usual, keep eating in restaurants, get out and keep the economy going, and so on, after cases and deaths had already started to climb. Oh, and churches that had services in which they encouraged people to hug each other.
I could go on and on, but all that will happen is that someone will say “the plural of ‘anecdote’ is not ‘data.'” So maybe I can sum it up this way: I’m almost 55 years old, I’ve lived in the United States my whole life, I’m familiar with the culture here, and I don’t trust enough Americans to voluntarily take the steps that are needed in the present circumstances.
Didn’t see this mentioned, but Sweden counts include both died WITH Covid-19 and died FROM Covid-19.
Not all countries do that. Given Sweden can count very well, I don’t think they undercount.
Source: https://reason.com/2020/04/17/in-sweden-will-voluntary-self-isolation-work-better-than-state-enforced-lockdowns-in-the-long-run/?fbclid=IwAR3NuNujEopPCN-pOuFFK7KtbKN9GH0pI95RzEJpv8rE2Mpz0lc7JRbxwhs
Sweden definitely undercounts on any given day: the total number of deaths announced as of today, April 20, is too low. But they will revise today’s number upwards over the next few days or the next week until it is accurate. By then, though, several days will have passed, so the number of deaths announced as of April 25 will also be too low, initially. And so on. This is an issue in every country, as far as I know, but seems to be larger in Sweden than other places I’ve looked at.
Birger (above) made the same point about Sweden counting a wider range of deaths, but I think the difference is not that big for at least some other countries. See my comment to Birger above. Or perhaps I should say: yes Sweden counts COVID deaths differently from some countries, but not all. Many other countries also count everyone who died with a positive test, or even everyone who died with symptoms consisted with COVID-19 even if they weren’t tested.
I am not convinced that the Swedish reporting lag (as opposed to the weekend effect) is greater than in other places, especially ones thad consider cause of death rather than diagnosis status in their reporting.
Does anyone know of any other country/state that reports the actual dates of COVID deaths (and ideally also their reporting dates)?
I don’t remember anyone including reporting dates but deaths by date are not that unusual. See for example New York City (daily counts chart in www1.nyc.gov/site/doh/covid/covid-19-data.page ) and Switzerland (page 6 in http://www.bag.admin.ch/dam/bag/fr/dokumente/mt/k-und-i/aktuelle-ausbrueche-pandemien/2019-nCoV/covid-19-lagebericht.pdf.download.pdf/COVID-19_Situation_epidemiologique_en_Suisse.pdf ).
That can accentuate the raw numbers but in terms of the *exponential rate of growth*, I suspect it might actually artificially shrink it. Basically other countries will see the death toll rise faster as health systems break down and more vulnerable populations are reached, but if in Sweden you add a fixed constant non-covid death rate to the infecteds, then that cushions the numbers.
In all these discussions people seem to be advocating an implicit underlying ideal curve for fatalities. It’s not clear what the justification for that curve is.
Maybe everyone doesn’t share Phil
Policy decisions based on minimizing one number (COVID-19 deaths in 2020) are very unlikely to be optimal for society. That simple fact seems to be more difficult to for some socio-political academic cohorts to understand or accept. It should not be that difficult to understand. Is it intentionally being misunderstood for political reasons?
Javier:
I don’t think anyone is talking about making policy decisions based on minimizing the number of COVID-19 deaths. I agree that this would be ridiculous. Indeed, it’s so ridiculous that I don’t think anyone is making this error.
Just want to clarify what some people have already pointed out;
Sweden cross checks all deaths reported (from all causes) with everyone who have been diagnosed with covid-19 in the last 30 days.
This means that if someone was diagnosed 29 days ago and died in a car crash yesterday, their death is still counted as a covid-19 death.
From what I understand, no other country has this wide a definition of covid-19 deaths?
Do you have a source for that?
It sounds like something someone has misunderstood.
“In Sweden, certifying a death has two stages. Firstly, the physician confirming a death immediately reports the death to the Swedish Tax Agency. This ‘notification of death’ (dödsbevis) is a legal obligation and must be completed before burial can be authorised. However, the cause of death is not included in this report. A second report, i.e. the medical death certificate (intyg om dödsorsaken), must be made to the National Board of Health and Welfare within 3 weeks of the death. Information from this death certificate and further information from the tax authority is recorded in the cause of death register (Box (Box1).1). The death certificate is usually completed by the patient’s usual physician or the physician last seeing the patient before death, and includes a version of the International Form of Medical Certificate of Cause of Death [4], which facilitates identification of the underlying cause of death.” — “The process for identifying the underlying cause of death is complex and is described in detail in ICD-10 [4]. In brief, the physician certifying the death is required to separate conditions that contributed to the death from other conditions that did not.” (“The Swedish cause of death register”, European Journal of Epidemiology 2017)
There are WHO standards for this! The idea that physicians would certify a cause of death, or contributory cause of death, that did not actually contribute, i.e. the idea that physicians would commit perjury, and for what? reaches into the realm of conspiracy theory.
They may not be looking at death certificates at all when compiling those daily reports. I don’t think that’s unusual.
It’s been clarified by the swedish health authorities several times durin their daily press conferens and reported in media as well, here’s one example from one or the biggest and most reliable daily news pappers (in swedish tho, Google translate is your friend) https://www.svd.se/lander-missar-coronadoda-pa-aldreboenden
What you quote is true as well and that is still how the procedure is in each individual case, but when it comes to calculating deaths from covid-19 they only look at the ‘notification of death’ database (which doesnt give cause of death) and crossreference with confirmed cases database. This can be done automatically and don’t require any extra man power. Meaning all deaths, no matter the cause, reported in sweden is crossreferenced to the confirmed cases database.
Belgium and France have a much wider definition, including possible cases not confirmed by laboratory tests (around half of the total number in the case of Belgium). And I don’t think people dying from other causes after being tested positive is going to move the needle much. There are 16000 cases in Sweden around ten would be expected to die in a given month, insignificant compared to almost 2000 deaths. The precise calculation would depend on the age distribution and other assumptions but you get the idea.
Is it wider, though? We now know that Covid-19 has a characteristic CT and X-ray (ground glass shadow), it is known how it affects the body and what it looks like when people die of it. If countries decide to let physicians determine the cause of death without a lab test, based on clinical criteria, maybe a post-mortem examination, why not? The objective is always the same: determine the cause of death accurately and responsibly.
Re: Sweden, I don’t see physicians going to the trouble of determining the cause of death twice. They’ll determine it once, and use the modern electronic system to report it, and that’s what the health office gets. I know that’s what happens in Germany, and given international standards for this, I doubt any particular country deviates much from that.
What motivation does a sane health system have to want to introduce that kind of inaccuracy into their records and statistics? The only reason is “they must be lying to us!”–“Why?”–“To control us!”–“How?”–“With lies!”
Wouldn’t be easier to just falsify the numbers instead of going through such an elaborate scheme?
I’m sorry, I don’t understand what inaccuracy do you think that is being introduced by who and when. In Sweden, as far as I can understand, a covid-19 death is reported if and only if someone who tested positive for sars-cov-2 dies. The cause of death in the death certificate is irrelevant.
The Belgian/French definition seems wider to me, because it includes people who dies at a hospital after being admitted with a sars-cov-2 infection and also people who dies at home or in a nursing home apparently from covid-19 even if no lab confirmation exists. I have no idea how do they determine which deaths to count, maybe it’s based on the death certificate. And I don’t know what happens precisely with someone who has an accident and dies because of it but had been tested positive for sars-cov-2. I think that even with those exclusion the definition which includes non-lab-confirmed suspected cases is wider.
As far as I know in Germany they also report lab-confirmed deaths only. And they doń’t really try to confirm suspected cases post-mortem, or at least they didn’t one month ago:
“Unlike in Italy, there is currently no widespread postmortem testing for the novel coronavirus in Germany. The RKI says those who were not tested for Covid-19 in their lifetime but are suspected to have been infected with the virus “can” be tested after death, but in Germany’s decentralised health system this is not yet a routine practice.”
https://www.theguardian.com/world/2020/mar/22/germany-low-coronavirus-mortality-rate-puzzles-experts
For your article from March 22, the key word is “currently”, we had 57 deaths at the time.
Further down the page, we learn that “Clinics dealing with respiratory illnesses have been on high alert about the virus for weeks, so I would be very surprised if there was a significant figure of uncharted deaths.”
You don’t just keel over and die from this virus, it’s not something the attending physician would be likely to overlook.
Is Sweden also publishing an accurate statistic of Covid-19 deaths, based on the full death reports?
I know that the RKI in Germany is doing that exclusively, but the delays involved are of course undesirable for some dashboard operators. I think the publicly available RKI data allows pairing cases and deaths, so I could probably get a true CFR for the older cases, by age group and sex, even.
“Clinics dealing with respiratory illnesses have been on high alert about the virus for weeks, so I would be very surprised if there was a significant figure of uncharted deaths.”
Other European countries have also been on high alert about the virus for weeks and that didn’t prevent a significant number of deaths from being ignored until they decided to widen the criteria. It’s of course possible that Germany it’s doing it better, but unfortunately they have not provided mortality data yet, as other European countries have done, so we cannot check how much of the estimated excess deaths are explained by the reported figures.
Sweden and Belgium indeed seems to be the countries with the most accurate calculations, however few other countries have the ‘personal number’ system. Its almlst impossible to be ‘lost’ in sweden as you need it to do anything really. Google is your friend if you want to know more but basically this means sweden numbers probably are more correct than most. From what ive understood no other country uses data as far back as 30 days, but i migth be wrong.
Regarding including non confirmed cases: almost all people who have any serious symptoms, in hospital or not, are tested before or after they die. The Labs still have free testning capabilities, thats why its possible to assume this (according to officials). I cant give you any english language source on this as it’s from the daily conferenses with the swedish health authorities, so i understand if you wont take my Word for it. However I think its safe to assume there Will be “false positives” in the officials covid death statistics, as car crash victims are included today, so maybe the non reported cases and The false positives cancel eachother out. I guess we Will now after this whole thing is over.
Heres data showing Sweden and Belgiums numbers compared to prevous years, showing both countries are probably doing their counting rigth https://www.nytimes.com/interactive/2020/04/21/world/coronavirus-missing-deaths.html
I don’t understand why do you find so relevant that people dying in car accidents may end up being counted as covid deaths. Say we had on average 10’000 people tested positive during one month at risk of dying from some other cause (there are more positives now, less in the past, some may have been diagnosed post mortem… looking at the curve It seems a conservative estimate). Say they have 5% chance of dying in a year (a very conservative estimate, as if they were all over eighfy!). You would expect 40 deaths. That’s a rounding error when 2’021 have been reported. I’m 100% sure that the number of cases undereported (who died due to covid-19 but nobody thought of testing, or didn’t want to for some reason, or where a false negative was obtained) is much higher than 40.
Did you even read the article? It clearly shows that the excess deaths in Sweden, compared to the avarage of the same period earlier years, adds up to almost exactly the same as the number of covid-19 deaths. For the period NY times looked at those numbers were:
Excess deaths: 1100
Covid-19 deaths: 1160
Thats MORE covid-19 deaths than excess deaths, so where would those unreported cases you talk about be hiding? Or do you seriously believe the Swedish government is somehow covering up a bunch of deaths, something that is pretty much impossible due to the swedish personal number system?
Belgium can also contribute their excess death toll to covid-19, good for then. France, on the other hand, has quite a larg number of unexplained excess deaths during this period, all of them wont be corona related but it’s pretty safe to assume many of them are.
“the average of the same period earlier years” is just that, an average. If you look at the chart the variation is half as large as the 2020 anomaly. And 2020 was tracking in the low end of that range until recently. The chart ends on April 12, the deaths have more than doubled since then. It would be interesting to see an update.
And what you get from that is an estimate of excess deaths, not some revealed truth. It doesn’t guarantee that no single covid-positive death has gone undetected. But you are free to think that the probability that someone who tested positive has died in a traffic accident (~0.025%) is higher.
I meant 2.5% probability (that someone reported positive died later in a traffic accident and was included as a covid-19 death).
No one said there wouldn’t be unreported cases or that NY times holds some all migthy truth. However, as I’ve explained, there are many things pointing towards Sweden having fewer unreported deaths than most other countries. Which is mainly due to the way Sweden keeps track of it’s citizents.
Judging from your insulting tone I doubt we have more to discuss here. We’ll just see who’s more accurate in a few months or years. Adios!
> For the period NY times looked at those numbers were: Excess deaths: 1100 Covid-19 deaths: 1160
I retrieved the data from scb.se, the last update is from a few days ago but the last days available are clearly incomplete. Earlier days may also be revised later. Looking at the changes between releases in the past, I think 100 additional deaths may be added for the period in the next release, still something more later.
The uncertainty in the excess deaths estimate is quite high. Calculated against each of those five years, excess deaths for the period are 766, 1337, 1332, 245 and 1749 (the average is 1086, that the NYT rounds to 1100). If they had taken the median instead of the average there would over 150 deaths unexplained. If they had taken just the last year there would be over 500 deaths unexplained. I don’t say those would be more meaningful results, I just say that it’s more a question of luck than accuracy that it was close to the average after subtracting the reported COVID-19 deaths.
Thanks for the details about the Swedish id number, by the way.
For the record, updated mortality data has been released. For the period considered (Mar 9 – Apr 12) there are 265 additional deaths. That brings excess deaths relative to the average of the last five years from 1086 to 1351. At the same time the official number of COVID-19 deaths has also been revised upwards in the meantime, to 1340.
> few other countries have the ‘personal number’ system
How is it different from the national ids common in continental Europe? (I exclude the UK, where i know that there is not, or there was not, such a thing.)
I wont be able to explain it properly, I’d suggest you google ‘personnummer’. I can however give you my personal experience: I’ve lived in Sweden, the UK and my home country of Spain so can only compare those. As you say UK doesn’t use this kind of system so I’ll leave that out.
In sweden the id number is used for e v e r y t h i n g – dealing with autorities, banks, applying for jobs, customer clubs, hotel reservations, marriage, signing contracts, renting homes/cars/anything, libraries, health care, education, paying, and so the list goes on forever. This, as well as being a well digitized country with centralized systems, makes it basically imposible to ‘hide’ or stay under the radar. It is widely criticised for infringing on the citizents integrity and eliminating privacy. In a pandemic, however, it’s quite useful to know basically everything about your citizents and tack them as Sweden does. It’s also quite convinient on an everyday basis living in sweden.
The Spanish (and UK) equivalent can’t even begin to compare. Main difference: it didn’t make my life easier (as the swedish does) and it doesn’t infringe on my integrity in the same way as there are too many systems that don’t connect.
This is obviously a highly personal explanation but it gives an idea.
Hang on, does this imply that they *do* not do additional tests of dead people to confirm if they have covid19? In other words the prevailing theory that “confirmed cases is an undercount but deaths are more accurately detected” is actually incorrect for Sweden because covid patients could be dying invisibly because they had no prior diagnosis?
In every country there will be people dying “invisibly” as not everyone is getting tested first. The degree of this happening may vary by country though.
They test post mortem and doctors can give covid-19 as cause of death without testning as well. However, cause of death is not the parameter used in the statistics over the corona victims, therefore these people won’t be a part of the death toll – today.
Seeing how well monitored Swedes are, I doubt there will be many invisible victims. My guess is the number of people who died of other causes but tested positive for covid-19, meaning they’re part of the statistics, will cancel out the ‘invisible deaths’. The graphs in this article seem to point to that as well https://www.nytimes.com/interactive/2020/04/21/world/coronavirus-missing-deaths.html
“The Swedish Public Health Agency made international headlines yesterday by estimating that one-third of Stockholm residents would be infected with the coronavirus by May 1. Less than 24 hours later, the Agency has taken a dramatic u-turn and withdrawn the report.
The decision was announced via Twitter: “We have discovered an error in the report and so the authors are currently going through the material again. We will republish the report as soon as it is ready.””
https://www.forbes.com/sites/davidnikel/2020/04/22/sweden-health-agency-withdraws-controversial-coronavirus-report/#2b9093434944
And the antibody prevalence study the Karolinska Institute did reportedly suffered from the problem that they included samples solicited from donors who had recovered from Covid-19 and donated pasma for use in antibody therapy trials.
It is striking to me that Sweden – a country whose population is by nearly every measure healthier than that of the United States – is experiencing a worse (per capita) COVID-19 death rate. Even as more than 2,000 die daily in the U.S., our rate cannot catch up to theirs. Perhaps it is just a matter of being a few days ahead of the U.S. but still, I would never have expected the two countries’ respective mortality curves to be growing essentially in parallel. That’s illustrative of the choice they’ve decided to make. Maybe it will finally pay in the long run, either via herd immunity or a healthier economy, but I don’t know.
The main thing Sweden has failed to do is protecting the elderly, especially in Stockholm. Compared to the US the swedish victims have a higher avarage age (Swedish health agency: https://experience.arcgis.com/experience/09f821667ce64bf7be6f9f87457ed9aa). This is explained to rather be due to the political rule in the Stockholm region (just Google Nya Karolinska hospital) than the Swedish approach to the pandemic. As well as a number of other parameters ofc. Will be very interesting to see what Will happen here (I’m living in Sweden, but not a Swedish citizent) and what the analysis Will give in the end.
Sweden’s population as a whole likely has a higher average age than does the US.
It’s a little older, but not as much as Italy, Spain or some others. Conversely, they are quite a bit lower than the US on measures like the obesity rate, and of course they do not have a substantial population without health insurance.
I think that trying to compare these outcomes across countries is more than anything else an exercise in confirmation bias
That said, my understanding is that a relatively high percentage of Swedes live in single-person households, and a high % are able to work from home.
Can we trust the US mortality figures?
Depends what you mean by ‘trust’.
If you mean ‘will deaths be intentionally covered-up’, probably not.
There are disagreements in the US (both between and within states) on how to count ambiguous cases (deaths with suspicious symptoms but no test confirmation, or deaths with confirmed COVID19 but an apparent other cause of death), however. This has led to allegations of falsification in the media and especially social media, but I kind of doubt that; I think there is genuine room for honest disagreement on these questions.
This also makes the statistics confusing as, for example, New York City reports several thousand probable-but-not-tested cases which the State of New York does not include in their own statistics…
Deaths are often reported several days or even weeks late (especially nursing home deaths, but others too) and deaths are also often (usually?) given by date-of-report vs. date-of-death, which makes the real curve of deaths hard to figure out.
But the total is going to be – while somewhat lagged – reasonable, IMO. Possibly somewhat undercounted relative to, say, Sweden since we probably have a greater undocumented population; but on the other hand, I’d expect many nations to have a much worse under-counting problem.
Time will tell. I noticed that the trend toward infections is going downward in Sweden and the people were more respected during this crisis. Virus cases do not matter as long as most recovered which they have here as well as there! It might give a vaccine to the rest who have no exposure and no possible immunity! Time will also tell if Sweden will have a relapse which is the “word” here. There is really no way to know if destroying our rights helped with the situation! I think the perspective is all too often political here! Democrats seem to want our economy to fail.
Not just for the economy to fail! They want all their friends and family to for as well!
Isn’t that obvious!
Rhonda:
Regarding your statement, “Democrats seem to want our economy to fail”: I think there is a real moral hazard here. The same thing arose in 2009 with the stimulus plan: Democrats controlled two of the three branches of governments, and Republicans in opposition had every political incentive for the economy to fail. Similarly when there’s a war, etc. It’s my impression that the parties usually limit their interventions to spin: the Republicans emphasized the bad in 2009 and the Democrats are emphasizing the bad now. I don’t know that either party in opposition was doing anything actively to try to make the economy worse, but there is some political conflict of interest. In Obama’s second term, it seemed like there were some active efforts by Republicans to sabotage the Affordable Care Act, but arguably they were doing this not out of a desire to make things worse, but rather because they thought the law was a bad idea. Similarly with various foreign policy interventions such as the reported efforts by Nixon and Kissinger to work with the South Vietnamese to stop peace from breaking out: this can be viewed as politically-motivated sabotage or some misguided goal of supporting an ally.
More generally, whenever there is a political opposition, there is a moral hazard that bad news for the country is typically good news for the opposition. I don’t know any way around this, other than the idea that the opposition hopes to be in power themselves some day. For example, if the Democrats feel confident about regaining power in any case, this gives them a motivation for them to limit any economic damage happening now.
I see similar claims being made all the time:
Democrats want the hydrochloroquine treatment to fail to make Trump look bad.
Democrats are rooting for the virus;they want the death numbers to go up to make Trump look bad.
Democrats want to keep people locked up so they can ruin the economy to make Trump look bad.
If you think in exaggerating, go to any rightwing online comments section.
There are variations on the theme:
Democrats don’t rant care about immigrants suffering, they only want their votes.
Democrats don’t care about poverty in the African American community, they onky want their votes.
It’s an old playbook:
Democrats didn’t want to limit terrorism because they didn’t want to hurt Muslims’ feelings, and they wanted to hurt Bush.
Thus kind of thinking is not distributed disproportionately across the ideological divide. Democrats engage in the same kind of rhetoric b
It originates from a toxic mix of identity agressive cognition and binary thinking
In other words, binary thinking makes it so that Trump fans can’t conceive that it’s possible for democrats to both want Trump to be hurt from a failing economy *and* not want the economy to fail.
Joshua:
I’m just saying that the moral hazard is real. How people act in the face of this moral hazard is another story.
Andrew –
I guess I’m having a hard time seeing how this fits under moral hazard.
My default is that Democrats don’t want the economy to fail. They want the economy to succeed – in other words, they want to be able to make more money, to reap the rewards of a rising stock market, to have their friends and family to be able to pay rent. There is *no* question about any of that.
They also want Trump to be hurt by a failing economy. It’s possible to have both desires at the same time. They aren’t mutually exclusive desires.
By the same token, my default is that Republicans don’t want people to suffer without healthcare. But sure, they wanted the ACA to fail. They wanted Obama’s administration to fail (and for sure, Democrats turned that into an argument that Republicans didn’t care about the health of poor people).
Seems to me that the notion of the moral hazard doesn’t work because it doesn’t account for the notion that people aren’t thinking in through the form of a logical flow chart.
In other words, the moral hazard isn’t “real.” It’s a construction in the minds of Republicans (in this case). It’s a product of framing, and a product of the toxic mix of identity aggression and binary thinking.
But sure, the perception of a moral hazard is real. The potential for people to interpret things in that way (because they are protecting their identity and are thinking in a false binary fashion) is real.
Joshua:
There are two moral hazards. The first is simple: The Democrats selfishly want power. If they can tank the economy, that increases their odds in the upcoming election: thus they can increase their expected power by hurting people. The second is more indirect: The Democrats selflessly want the country to be a better place. If they can tank the economy, that increases their odds in the upcoming election, and if they win the election they can do good things for people.
Both these moral hazards are always there for both parties. When the Democrats are in power, the moral hazard is on their side.
Andrew –
> The Democrats selfishly want power. If they can tank the economy, that increases their odds in the upcoming election: thus they can increase their expected power by hurting people.
If they could simply extract tanking the economy, that might be true. But they can’t. Tanking the economy means that they suffer. Their friends and family suffer. It’s not like people aren’t aware of that. Of course they are. In some abstract form they’d like to tank the economy if they could do so, but they know that no abstraction such as that exists. So Republicans go with the abstracted form and interject it into the minds of Democrats and come up with “You want the economy to fail just to hurt Trump.”
Sorry, that should be…
In some abstract form they’d like to tank the economy if they could do so *(without suffering, without their friends and family suffering)*, but they know that no abstraction such as that exists.
Andrew –
Not wanting to beat a dead horse but…
The more I think about this, the less I understand your position.
It is very much because Demz are *not* protected against the risk of an economic downturn that this *does not* seem like a moral hazard scenario to me.
For the sake of example…let’s say that I have a trust fund, and my friends and family have trust funds as well. And so we are all impervious to an economic downturn. And I really, really hate Trump. And I don’t care about poor people or anyone who might be hurt by an economic downturn.
And so then if given the chance, I could choose to do something to hurt the economy in order to hurt Trump. And so that would be a moral choice I might make. There are moral implications to caring more about hurting Trump than caring about the suffering my action to harm the economy might cause to other people. And I am protected against risk. And that would seem to me to fit the descriptor of a moral hazard.
But short of such a weighted scenario, I wouldn’t be in the position of making some kind of moral choice to hurt Trump and hurt other people and still be protected from risk.
To offer a personal scenario. Much of my income currently comes from collecting rent. A few of my tenants have taken a big hit to their income, and their ability to pay rent is in jeopardy.
1) I would love it is Trump’s chances of reelection are hurt by an economic downturn.
2) I most definitely don’t want a continued economic downturn because it will mean I’ll have to dip into my savings in order to pay my bills, maintain my lifestyle, etc. Also, I like my tenants and don’t want them to be unhappy. I don’t want to have to find new tenants if current tenants can’t pay rent. Etc.
I am not protected against the risk of an economic downturn. I can not decide to contribute to an economic downturn and be protected against he harm that would follow. But yeah, I hope that an economic downturn prevents Trump’s reelection.
And truth be told (please don’t let this get out), I’d actually not want to see more widespread suffering, even among Republicans :-)
It fascinates me learned folks posting here are simply ignoring the fact we literally have very similiar genetic, socially organized, culture, geography, health care systemics and economic models literally right next to Sweden. We have their Scandavian neighbors. We see a huge difference in death rates and infection rates. To discount demographics between NYC and LA is simply a fool’s errand. Epidemiological comparative modeling has standards. Its the same reason we would be my prone to do a sickle cell test on an African American with certain symptomatics than we would one Mandarin genetics. We have the models. We have seen an exponentially huge difference between policies in Scandinavian countries. Public policy is the most glaring difference. Food for thought.
I also find it odd that politics and conspiracies are being discussed on a Columbia website. Its seems politcal paranoia is immersed into academia as well.
Timothy:
I’m in the political science department; of course I discuss politics! Regarding “paranoia,” you’ll have to be more specific.
Some information that might help prevent comparisons to Sweden from being overly-simplistic reverse engineering that neglects confounds as people scramble to confirm ideological biases about “lockdowns.”
> (3) Concerning Sweden, Die Welt (in German) looks at what it calls the Swedish Sonderweg (“special road [taken or followed]”). Notably, it does not attribute the much higher mortality (compared to fellow Scandinavian countries) just to its not entering a lockdown (some voluntary social distancing measures are in place) — but to the “limping” Swedish healthcare system (marodes Gesundheitssystem).
They are at pains to point out that this is not a matter of money — Sweden has the 2nd highest pro capita spending in the EU, after Germany — but of inefficiency, administrative bloat, and wastage. Once upon a time, Sweden had 49.5 ICU beds per 100,000 inhabitants, which today would be the highest in the world, above even the USA. Today? Just 5.8.
Even before the COVID19 crisis, 12% of elective surgery patients has to wait 4 months or more, compared to 2% in France and none at all in Germany. One-fifth of Swedes have to wait more than 2 months for a specialist appointment, compared to only 3% in Germany.
Much like Israel’s public system, rapid access for life-threatening emergencies in Sweden is maintained at the expense of ever greater delays for everything else. [But much unlike Israel, Sweden entered the present crisis without the benefit of a young population and a warm, sunny winter and spring climate…] Doctors in the public system are salaried employees of the state, with all that entails in terms of (lack of) incentives…
https://spinstrangenesscharm.wordpress.com/2020/05/12/covid19-lag-ba-omer-edition-active-cases-graphs-around-mostly-europe-more-sophisticated-model-predicts-much-smaller-herd-immunity-thresholds-swedish-healthcare-problems-n-acetylcysteine/
Meanwhile…in Sweden…
People really should try to resist making comparisons related to COVID-19 before enough longitudinal data have been collected.
I’m not particularly critical of Sweden’s approach. It’s one of the variety of bad choices.
But when you look at the metric of deaths per capita, you will note that the rate of decline in Sweden is considerably lower than in Switzerland, the Netherlands, even France, and many, many other countries. Sweden is rising up the chart at a consistent pace.
In fact, Sweden has had the higher per capita deaths in Europe over the last seven days. Even higher than the UK.
Cross-country comparisons are of limited value. And the reasons for Sweden’s relatively slower decline than elsewhere are complicated. And there are necessarily tradeoffs in all of this, but you can’t even evaluate the tradeoffs if your vision is limited by your ideological blinders.
Yes, this is all correct.
However, I do think it is meaningful to point out that Sweden has not seen hospitals overwhelmed and really high death rates as were predicted by some of the models in March and early April, though it clearly not done as well as surrounding countries.
I really don’t see a path for Sweden to end up with, say, .35% of the population dead (which is what the Imperial College model’s limited mitigation prediction of 1.1 million for the US would equate to).
So, I’m calling up the great data explorer on ourworldindata.org…
https://ourworldindata.org/coronavirus-data-explorer?deathsMetric=true&totalFreq=true&perCapita=true&smoothing=0&country=USA+GBR+CAN+BRA+AUS+IND+ESP+DEU+FRA+SWE
So far, in about 2 months sweden has ~ 375 deaths/million, and your 0.35% is 3500/million. So if their epidemic continued in its fairly linear fashion for 20 months, they’d get there.
now, the Imperial College model assumed that limited mitigation would result in much faster growth than what has been seen in Sweden. With faster growth comes less good health care, and health resource depletion. I don’t believe that the IC model had seasonality built into it, and there does seem to be some level of seasonality. If seasonality *is* playing a role, then this fall will be a disaster.
Note, the swedes themselves don’t think that they’re doing “limited” mitigation, most of the stuff we’re calling “shelter in place” is going on there according to what is reported here https://www.washingtonpost.com/world/2020/05/12/swedens-coronavirus-strategy-is-not-what-it-seems/ the main difference is whether things are government MANDATED or simply encouraged “A key distinction for Sweden is that its government believed it didn’t need to enforce guidelines regarding social distancing on a population that would heed the advice of the country’s independent public agencies. According to polling data, Swedes have a high level of trust in the country’s public institutions.”
Basically the US is about to enter something like a Swedish model where stuff is open but for more limited gatherings and contact levels. Sweden’s continuous rise in deaths shows that we are likely to see the same here in the US.
From what I understand. the problem in Sweden is centered to a large degree in nursing homes. This is also true of the US and other countries that have imposed lockdowns.
We may be overthinking the importance of restrictions on the general population and underestimating the importance of protecting nursing homes, which are 1) enclosed spaces, 2) have dense populations in proximity and 3) have at-risk populations.
I think the nursing homes are always going to be early problems. But we have months and months to go. In my opinion, this first wave we’ve experienced is just the start, and it seems very likely there’s a seasonal component, and that the real problem for the general population will hit around next september.
I don’t see why a fall second wave would be worse than this one.
Treatments will be better (it looks like ventilation was not managed well in NYC and other early-hit places; remdesivir will be widely available; we might have something better [monoclonal antibodies?] by then…)
Spread should be slower since the high-density and probably most vulnerable areas have some immunity, so R will be lower (NYC ~20% – higher in some areas, Boston city 10%/Chelsea 30+%, etc…. other places that have been very hard hit like New Orleans and Detroit are likely comparable, though we don’t have serology studies from them).
The second wave was much worse in 1918-19, but that seems to have been due to WWI specific issues that don’t apply here.
“I don’t see why a fall second wave would be worse than this one.”
Because some people are addicted to predicting disaster and when their predictions turn out to be overblown, they just double down with predictions for the “next wave”.
Kind of like the whole “lockdown early, lockdown forever” true believers. Their belief is utterly un-falsifiable. If a whole lot of people somewhere die (like in NYC) it’s because they didn’t lock down hard enough or early enough. If the death rate is more reasonable, that’s because whatever lockdown was done managed to avert disaster. No matter what happens, their answer is “lockdown”.
It’s like a sick version of the old SNL sketch about “more cowbell”.
Brent –
> Kind of like the whole “lockdown early, lockdown forever” true believers
I questioned you about this rhetoric before. You didn’t bother justifying it then.
Should I assume asking you to do it now will have the same result?
Brent:
You might read this:
https://julesandjames.blogspot.com/2020/05/blueskiesresearchorguk-why-cant-germans.html
and this:
https://julesandjames.blogspot.com/2020/05/blueskiesresearchorguk-human-cost-of.html
Of course we can’t wind back the clock to falsify his model results, but if it is handwaving it’s a higher level of handwaving than you’re providing. Maybe you should go over there and try convincing him that there’s no evidence for the relative effectiveness of lockdown at different stages of the epidemic.
Brent clearly lives in Fox News World, where radlibs and feminazis were slavering for permanent lockdowns to get what we always want, which is power over white guys, who are always and everywhere the Real Victims in All of This (TM). Best ignored at this point.
Kyle:
That is not helpful!
I should not respond to Kyle C’s characterization but in the interest of full disclosure…
My lifetime exposure to Fox News is on the order of 5-10 minutes, if that. And while my political views are mainly dismay at the entire system regardless of party, as it happens I have voted against every Republican candidate for national or state office these past three decades plus. With the exception of Barack Obama I can’t honestly say I have “supported” any candidate, my voting is generally anti-right rather than pro-left.
When I object to this or that bit of self-justifying circular reasoning, I am not making a crypto-political point. I am probably the least political person that I know.
Well, here in CA we did all the right things, we were the first ones to issue safer at home, we did so Mar 19 at a time when there were only really a handful of cases, and we’re at ~ 5% seroprevalence today. We’re reopening more now, even as cases per day have been trending upward. There’s a slight indication of leveling over the last week or so. If there’s seasonality in this virus, and people get used to over the summer doing things relatively safely… my concern is we will carry that into the fall and have the wrong adaptations for the fall increase in severity from seasonality.
The long history of seasonality in respiratory viruses tells us that the fall is the big time when everyone gets sick from respiratory viruses… so it’s hard to move away from that prior without some strong evidence, and of course we don’t have any strong evidence of anything. Rational thing to do is to assume the summer is safer and that the fall is not.
Beyond the viral spreading issues. It’s hard to know, because we’re talking about human behavior, but I think there’s in general a natural tendency for people to let their guard down, and make decisions about the future based more on what they see today rather than projecting into the future. Suppose the public health industry says “the fall is coming, we expect a lot more transmission, large swaths of the population should take their vitamin D and return home and stop working for a few weeks while we assess the changes in transmissibility “… how are people who’ve been doing fine for 2-3 months going to respond to that?
That’s my main concern about the fall.
CA is potentially more vulnerable, yes, because there are some very large cities that are fairly dense. And since CA locked down quite early it might be less affected per-capita because of that, not because it’s inherently not very vulnerable.
I’m not as concerned for the fall about TX (where I am) or other relatively populous Southern states like GA and FL, since they locked down fairly late and not as comprehensively, so I think we would have seen worse outcomes if they were going to happen. In mid-March the news was predicting disaster for FL and TX because of Spring Break, saying that those states would be “the next Italy”… totally didn’t happen. Houston and San Antonio are among the least-affected large cities in the US (Harris County is less than 50 deaths per million, Bexar County under 35).
I agree that people in many parts of the US will be less careful in the fall… I just don’t think it will be all that big of a disaster.
People in the really hard-hit places probably *will* be careful, and some of them will have high enough immunity to make a meaningful difference to the R. A lot of the rest of the US was probably not at that much risk of really explosive growth to start with.
There will probably be some places that fall in between, and thus are hit worse in the fall than they have been so far. But I think the *US overall* will be better off.
confused said,
“Houston and San Antonio are among the least-affected large cities in the US (Harris County is less than 50 deaths per million, Bexar County under 35).”
Houstonians may have gained enough wisdom and humility from the last two hurricanes to refrain from overconfidence and prepare to face non-meteorological challenges as well.
It could be… though learning from hurricanes really doesn’t fit very well with my experience (I lived there until a few years ago)…
I feel we may be focusing too much on the 1918 pandemic. It may offer us a potential worst-case scenario, but I’m not sure how likely it is. Science has obviously advanced a great deal since that time, we don’t have the major factor of soldiers returning from war, and this also isn’t influenza but a coronavirus.
Generally, virus mutation tends to be in the direction of less lethality. I do think there will be some seasonal component to this virus but it seems unlikely that it would mutate to become more lethal, except perhaps in isolated areas. A second broad wave would probably be of a less deadly (and more infectious) strain.
Yeah, I agree 1918-19 is not the best model for a number of reasons. It seems like the fact that the second wave was worse than the first was due to WWI-specific and possibly influenza-specific factors, so probably won’t happen now.
The pattern may look different since in 1918-19 global travel was slower, but there is more social distancing now.
If there is seasonality (and some level of seasonality seems plausible, a priori, since most respiratory viruses – including common-cold coronaviruses – show it), then a second wave of some sort is likely, but not necessarily a worse one. It might be milder, since the most vulnerable areas (NYC, Lombardy, etc.) have enough immunity to reduce R somewhat.
I think there’s unfortunately a lot of confusion in the media between a “resurgence” driven by relaxation of measures, and a “second wave” which is inherent to the virus, seasonality etc. If there is a spike in June (in the Northern Hemisphere) that’s a resurgence; if it happens in October or November it’s much more likely to be a genuine wave.
>>So far, in about 2 months sweden has ~ 375 deaths/million, and your 0.35% is 3500/million. So if their epidemic continued in its fairly linear fashion for 20 months, they’d get there.
Yes, exactly. But Sweden predicts they will be at herd immunity pretty soon – I’ve seen June quoted. So if that is true they will have 1-2 months more and stop with maybe 2x their current deaths.
I’ve seen other arguments that that is wrong and Stockholm is more like 10% infected than 30%.
But even if so… a 10x increase in deaths would mean 100% infected, which isn’t plausible. In a relatively low-density place the R0 is probably not as high as usually quoted and thus the herd immunity threshold would be lower (and some papers/preprints suggest that contact networks mean that the usual 60-80% predictions are too high anyway).
>>now, the Imperial College model assumed that limited mitigation would result in much faster growth than what has been seen in Sweden.
Yeah. And this is even more dramatic in rural parts of the US. Now I think South Dakota closed schools, unlike Sweden, but still, it’s pretty dramatic. South Dakota had one big outbreak around Sioux Falls (associated with a meatpacking plant) but it doesn’t seem to be expanding further very much, they seem to be past the peak (3023 of 4177 cases are recovered).
And it stayed pretty localized… the 700,000+ people in the rest of South Dakota have seen a total of 6 deaths (40 out of 46 deaths in SD are in Minnehaha County).
I am wondering if the issue is that the Imperial College model only had data from Wuhan and maybe Lombardy to work on… and both regions are very dense compared to Sweden, much less South Dakota.
So the R0 in moderate-density to very rural areas may be a lot lower than the model would suggest, and thus the “herd immunity” threshold/final % infected would be a lot lower as well.
NYC did see over 2 deaths per thousand, so 0.35% of the population dying with limited mitigation seems very plausible for dense population centers. Just not for other places…
>> If seasonality *is* playing a role, then this fall will be a disaster.
I don’t know… R will be lower then since a significant percentage of the population will be immune from this “wave”, plus lethality should be less due to better treatments (most developed world countries will probably have lots of remdesivir by fall, and maybe something better… monoclonal antibodies?).
>> Sweden’s continuous rise in deaths shows that we are likely to see the same here in the US.
I don’t know. Some places probably will, but the US overall?
I think there are at least 3, possibly 4, categories of places in the US that are going to have different patterns.
– Hawaii and possibly Alaska (and Virgin Islands/Guam) where eradication of the virus is reasonably possible, but they will have hard choices about how to “open up” to the rest of the US;
– very rural areas in the contiguous US: most of the Great Plains, except for occasional localized outbreaks related to prisons/meatpacking plants/etc. I don’t see an obvious reason for that pattern to change; it may get a bit worse as things reopen, but I think South Dakota and Arkansas (no stay-at-home orders) should have had major problems by now if they were going to.
– Midwest and Northeast urban areas; already very hard hit. Fall wave could be very bad, but in the worst hit places, there is enough immunity to blunt its impact (lower R); treatments should be better/more available, knowledge on how to manage patients will be better. And the worst hit places are probably not random, but more inherently vulnerable, so I doubt we will see another NYC-level situation in the US.
– The areas that might see worse trouble are those in between, that could have been hard hit but weren’t, due to some combination of luck and taking measures early.
Ugh, I messed that up: the second kind of places in the US was supposed to be “very rural areas in the contiguous US: most of the Great Plains, the northern mountain states (ID/WY/MT), Maine/Vermont, Arkansas: these places have been very lightly affected except for occasional localized outbreaks related to prisons/meatpacking plants/etc.”
LA is one of the hardest hit regions of CA, and the seroprevalence study published today by the Santa Clara/LA guys suggested 2-7% with about 5% best estimate. CA has over 10% of the US population, and essentially everyone is still susceptible.
you are 100% right about highly rural areas having more limited risk… PARTICULARLY if churches and sports and other superspreading risks remain closed… but it’s also the places where armed protesters are demanding their religious freedoms and congregating at bars to celebrate reopening etc… meh.
I’m concerned about CA and particularly socal and sf bay and maybe Sacramento. similarly Portland and Las Vegas and Denver etc
Daniel:
CA is putting a massive contact tracing effort into place. A large number of state employees are being trained and assigned to this task for a couple of months at least, with plans to hire people to replace them as their absence from their normal assignments starts hurting agencies too much. Contact tracing will be managed online using an adaptation of a very popular cloud-based suite of software normally used to track sales leads as they progress through the sales process. Online training has been rolled out and state employees already are interfacing with county health departments, getting the process up to speed, getting training started.
I’m cautiously optimistic about the Bay area and Central Coast (where I live), which has been and I believe will continue to be aggressive about controlling this.
SoCal … I’m not so optimistic.
I am glad to hear this, I had heard the talk, but hadn’t heard much about what actions were actually being taken. I assume you must know some people participating in these efforts. so that’s good.
SoCal is where I live these days, and SoCal alone is bigger in population than the smallest… like around 10 states put together. People keep talking about how the US is doing, but the US is basically CA, TX, FL, NY, PA, IL, OH, GA, NC, MI, NJ, VA, WA, AZ, MA
that’s like 213M people out of 330 ~ 65%
If you want to talk about where are *people* at risk, there is plenty of risk to go around in those states still…
Daniel:
Yes, I know someone with the state who is currently working seven days a week on this.
The six bay area plus santa cruz and monterey counties saw new cases drifting down until about two weeks ago, now they’ve plateaued. However, testing is exploding. Here in Monterey County now everyone can get a test, no doctor referral needed, no symptoms required. Not sure what’s going on that way in the Bay area except obviously testing is increasing. So that leveling off of new cases might be, in part, due to testing.
There are some small-scale revolts going on here in Monterey County, with a restaurant opening in defiance in Carmel, no social distancing, neither staff nor customers wearing masks, and a handful of other businesses are opening in the next couple of days it appears. The restaurant owner has been slapped with misdemeanor charges, which he has ignored, and there was a rally supporting him at the restaurant over the weekend. With people from San Jose etc who have also been demonstrating in Santa Cruz for their right to use Santa Cruz beaches. So it’s starting to get a bit ugly, but overall there’s support for continuing rational measures to keep things in check.
We shall see what the future brings.
shelter in place was always supposed to be until such a time that testing and contact tracing could keep the reproduction number down even while people shifted to more openness with physical distancing in public with some rational stuff open and the scary stuff still closed (like choirs or football games)… but except for CA, it seems like contact tracing effort is nowhere to be seen. It’s like you’re bleeding in the waiting room of the ER and they say “hold this compress on it until we can get the doctor to come take care of you” and then the staff goes off and drives home and goes to bed.
The compress wasn’t the treatment…. get the damn treatment here ASAP!
I don’t live in California, but where I am, the stay-at-home order was justified as a means of “flattening the curve” – i.e., protecting hospitals from a surge of COVID patients. This has come to pass; most hospitals are actually well below capacity at the moment.
I’m not sure about contact tracing; I think we are too late in the game for that to realistically work. But following best practices (wearing masks, keeping safe distance) will help. There seems to be evidence that viral load is a factor in the severity of the virus. A mask might not prevent exposure but could reduce your viral load, giving your immune system a better chance of fighting it off.
John,
contact tracing at scale can work. I agree that if you just trace 1/100 people, it’s a waste of time, but in CA we have ~ 1700 new cases each day. If we have 10,000 contact tracers they can track down most of the closest contacts of each person each day. If this reduces the reproduction number substantially below 1, then the infections per day begin to decrease exponentially on their own. Within a few months or so you could be at the point where there are 100 per day. If there are 100 ascertained COVID infections per day, the world is a way way safer place for people to go about their more normal daily lives, and the economy and people’s personal lives become far far more vibrant.
I think when you say it’s “too late in the game for that to realistically work” you mean it’s too late to eradicate the virus that way. and THIS I agree with, but it’s not too late to suppress the virus to something that affects only a tiny minority of unlucky or high risk people. The mathematics of exponential decay make that easier and easier as time goes along.
Then, when fall comes, and things get more infectious, the contact tracers have to work harder but we don’t get exponential growth, just a bit more work for the contact tracers.
Again, I think this comes down to people misunderstanding the whole idea, and giving up on it out of ignorance. Testing and Contact tracing is HUGELY successful and the entire reason why S Korea and Taiwan are doing fine with only a handful of cases per day.
Furthermore, given the long tail on the contact distribution, if our current contact tracing capacity just focused on the people at most risk of being super-spreaders, it might well be effective at much lower numbers of contact tracers, like the first thousand they hire in CA might be enough to really make a huge down-turn if we were smart about it.
Some people are being dumb in those areas, yeah… but I don’t think they are actually that big of a fraction of the population (they just get on the news)… and I doubt it will change much.
South Dakota had one huge outbreak associated with a meatpacking plant but it seems to be dying down, and the rest of the state hasn’t been hit hard at all… If it wasn’t for the media, they probably would never have noticed there was a problem (6 deaths among 700,000+ people outside the Sioux Falls area). And SD has the least measures in place of any state, though still not at “normal life”.
Any outbreaks that might occur from a bar or protest in these rural areas will probably die down in the same way.
> Sweden predicts they will be at herd immunity pretty soon – I’ve seen June quoted
Giesecke expects Stockholm to reach herd immunity (40-60% rate of infection) by early-June. Maybe he’s right, but one month ago he expected that it would be achieved by mid-May. And he assumes prevalence in Stockholm is already over halfway there, which is far from clear.
The current situation in Stockholm may not be very different from Madrid or Milan and no-one expects herd immunity there in a matter of weeks (but it’s true that infection is now spreading faster in Sweden than in most European countries). Most of the Swedish population is not living in then Stockholm area, by the way.
A summary of the Swedish case, with lots of references: https://www.foreignaffairs.com/articles/sweden/2020-05-20/swedens-coronavirus-strategy-should-not-be-worlds
Carlos –
So supposedly Stockholm was at @7% in late April. They are saying that projects to 20% now. I’m dubious, given that doubling rate is probably LOWER now than during peak times during Feb – late April, and thus I question whether 2+ months to get to @7% (first case was Jan 31) goes to 20% in slightly under a month, even with exponential growth.
https://www.reuters.com/article/us-health-coronavirus-sweden-strategy/swedish-antibody-study-shows-long-road-to-immunity-as-covid-19-toll-mounts-idUSKBN22W2YC
indeed, Sweden seems to be in linear growth based on graphs at 55/million per day. So 7% in late April means say 30 days times .000055 means an additional 0.16% of course this is Sweden wide… so maybe if all the growth was in Stockholm we multiply that by up to 10, since about 10% lives in Stockholm… so they are at 8-9% in Stockholm maybe?
I guess you have to account for ascertainment. so if they underascertain by a factor of 10 and you factor in all the rest. you can get to 17% but it’s a stretch. I’d guess more like 10-12%
which just goes to show that seroprevalence data is really needed on a rolling weekly basis. I imagine the swedes would be in a good place to do randomized sampling using the personnummer and get compliance. with around 1000 sampled per week they could be really on top of this like no other country. I wonder what’s really happening with seroprevalence surveillance
Daniel –
By “ascertainment,” are you referring to the lag between infection and when antibodies show up?
If you look at that video I linked in the other thread they present a nice breakdown of the timeline for that. IIRC, at around 38 minutes in or so.
[April 21] “Around one-third of Stockholm’s 1 million people will have had the novel coronavirus by the start of May and the disease may have already passed its peak in the capital, Sweden’s public health agency said on Tuesday.“
[April 22] “Tegnell said sampling and modeling data indicated that 20% of Stockholm’s population is already immune to the virus, and that “in a few weeks’ time we might reach herd immunity and we believe that is why we’re seeing a slow decline in cases, in spite of sampling (testing for the coronavirus) more and more.”
[May20] “Sweden’s state epidemiologist, Anders Tegnell, said the antibodies figure was “a bit lower than we’d thought”, but added that it reflected the situation some weeks ago and he believed that by now “a little more than 20%” of the capital’s population had probably contracted the virus.”
“is a little bit lower (than expected) but not remarkably lower, maybe one or a couple of percent,” Tegnell told a Stockholm news conference. “It squares pretty well with the models we have.”
It does seem remarkably lower compared to what he, and his models, said four weeks ago!
so on April 21 they thought 33% of Stockholm, then April 22 they thought 20% of Stockholm, and then almost a month later, May 20 they are still predicting that “any moment now we’ll hit 20%”… so basically they haven’t got a clue…
Daniel,
Anders Tegnell has a model. Everybody nowadays has a model. Some models say it’s the end of the world, some models say Stockholm is 20% prevalence.
Nobody has a clue at this point, just models.
To paraphrase the Steven Hawking story about turtles, it’s models all the way down…
On April 21/22 they said it was 20% by then and it would be 30% by May 1st. That part is coherent. On May 20 they said it was 7% by May 1st and it is 20% by now.
brent, Lakeland has never yet conceded a point in the history of Gelman’s comment section; don’t get your hopes up that you will be the first to get him to do so.
Carlos –
> That part is coherent. On May 20 they said it was 7% by May 1st and it is 20% by now.
Yes, that makes the timeline more plausible. Number for late May reflects infections for two weeks earlier (I’d say more like May 7th than May first). And the 20% now isn’t seroprevalence but actual number. So that makes it more like 7 weeks to go from 7% to 20%.
Oops.
Number for late *April* reflects infections for two weeks earlier (I’d say more like April 7th than April first). And the 20% now isn’t seroprevalence but actual number. So that makes it more like 7 weeks to go from 7% to 20%.
I didn’t think it could happen, but now I think it’s starting to look like Sweden may eventually have more per capita deaths than Italy (they already passed France).
Lots of reasons why that may be the case – not likely simply a product of the policies in government mandated shelter in place orders. Seems that they have a rather casual attitudes towards treating infected older people which is certainly a contributing factor.
But, folks may want to start backing away from the idea that Sweden should be a model for the U.S.
Especially if a vaccine is distributed on a moderately fast time table.
Sweden isn’t a very good model for the US anyway, it never really was. Nor was any other country suggested … Singapore and South Korea have a vastly different culture and attitude and are ‘effectively’ islands (not much transit across Korea’s only land border), plus they are tiny in comparison. (Singapore has a smaller population than my metro area, and actually has more cases, though significantly fewer deaths.)
There really is no good model for the US. The only other countries with comparable size, population, and internal regional differences either have vastly different forms of government (Russia, China) or very different economic situations (Brazil, India).
On the other hand, ironically, those states that followed a “low action” model seem to be doing notably better than Sweden … probably because they don’t have a Stockholm-sized city?
South Dakota did less than any other US state, and has a relatively low population fatality rate (currently less than 1 per 10,000). And the situation seems to be improving somewhat, though slowly (Of course this is highly dependent on testing…)
Now, even South Dakota did close schools, unlike Sweden – but it’s mid-June now, school year would be over even in a normal year.
I have said over and over that I don’t think that cross-country comparisons are very useful. Too many variables for which you have no control. Then add in how you should only be comparing after you have high quality evidence collected over an extended time period.
But comparing across states is likewise fraught.
The most obvious problem with such comparisons is one logic. Different localities enacted different policies precisely because of the different characteristics of rhe different localities. Right from the jump you are presented with a reason why comparing outcomes and thinking they result from different policies rather than different starting conditions and different basic, intrinsic attributes (like population density or willingness to wear masks, ability to work from home, % of single-person versus multi-generational households, etc.) is a dubious conclusion.
Like this:
> South Dakota did less than any other US state…
Part of the reason why they did less is because they had less of a need to do anything. So right off the bat, comparing it to states that had more of a need (say because of more international travel, higher density, better healtjcsre infrastructure etc. or for reasons we just can’t pinpoint) is fraught and likely a process of confirmation bias as much as anything else. And be particularly careful if you might have an ideological bias or even a reputational cost or sense of investment (because you wrote blog comments weighing voicing an opinion, or even just because you thought to yourself a particular answer was correct) aligned with a particular conclusion.
You are the easiest person for you to fool.
Joshua said,
“Part of the reason why they did less is because they had less of a need to do anything. So right off the bat, comparing it to states that had more of a need (say because of more international travel, higher density, better healtjcsre infrastructure etc. or for reasons we just can’t pinpoint) is fraught and likely a process of confirmation bias as much as anything else.”
So this sounds like a situation that illustrates how drawing a diagram of plausible causal pathways would be important in designing an appropriate model.
>>Part of the reason why they did less is because they had less of a need to do anything.
I actually agree!
I was not saying that South Dakota is a good model for the US as a whole. I was just using the comparison to question why there is so much focus on Sweden, since low-action strategies are being practiced “closer to home” and showing death rates per capita lower than Sweden’s.
Neither Sweden nor South Dakota is a viable model for, say, New York, California, etc.
We should keep in mind a couple of things.
First, different countries report COVID deaths differently. Sweden is known for being fairly transparent in its data collection, which has earned it an unfair reputation at times (it has been dubbed the “rape capital of Europe” because it reports cases that might not be elsewhere). So this may not always be an apples-to-apples comparison. (Belgium may be suffering on these charts for similar reasons.)
Second, the main problem in Sweden – as in so many other places – has been inadequate protection of retirement homes. This has happened across a range of countries following different COVID policies and it is uncertain how related it is to Sweden’s keeping its economy open. Most in retirement homes tend not to be actively circulating in the general population.
I believe that Sander Greenland cautions against drawing comparisons and contrasts across countries. I agree with that posture.
Protection of the vulnerable has been the whole thrust of closing economies. It was predicted that it would not be possible to (meaningfully) selectively protect populations such as those in nursing homes if the virus circulates at high incidence levels throughout the broader population.
This concern has been borne out in Sweden and other places.
Saying the “main has been inadequate protection of retirement homes” is akin to saying the “main problem has been too many vulnerable people catching the disease and dying”.
Joseph –
Yes. So often I read people say we should just “protect the vulnerable” and let the yuong and healthy get infected to reach herd immunity.
Protecting the vulnerable is easier said than done, especially with a higher prevalence of infected people running around. And often people who are making that argument don’t realize how many older people can’t realistically isolate because they have to work, go shopping, go to the doctor, take public transportation to get around, etc. I think ignorance of what life is like on the other side of the class and race/ethnicity divides help to explain why people make an argument that is so unrealistic.
Adding to the problem is that there are millions of grandparents acting as the primary caregiver for their grandchildren in this country, or at least living in multi-generational households. And the prevalence of such households is greater in lower SES communities. Again, I think a lot of people take for granted how difficult it is to “protect the vulnerable” because of a lack of life experience so as to understand how many vulnerable people live.
All good points.
Fair. But note it doesn’t require personal experience to be aware of the risks; there were plenty of experts making this point if people/governments were willing to listen.
For example, the ICL March 16 paper predicted 500k UK deaths in an unmitigated epidemic, and that that could be reduced to 250k if the UK were to take low-pain measures with a focus on protecting the vulnerable (specifically, locking down people 70+, plus locking down people known to have active infections and their housemates).
A 50% reduction in deaths is nothing to sneeze at, and while presumably that savings came mostly from selective protection of the elderly, it was nowhere near what could be accomplished by countrywide lockdown, which was predicted to push deaths all the way down to 20k. In that case, it was drastically reducing overall (rather than selective) infection prevalence that led to the significant savings of lives, although again it would mostly be in the elderly cohort that lives were saved (since they would make up the bulk of the deaths in the other scenarios).
Although the UK did lock down, largely due to those predictions, and is well past 20k deaths (over 40k now…)
Now, that might be because it wasn’t done well enough or relaxed too soon, and there’s likely some truth to that. But I think their “no action/limited action” numbers were too high and their “lockdown” numbers too low (for UK/US at least… South Korea, Singapore, etc. are a quite different story).
The UK population is ~67 million. 250k is ~0.37% of that, 500k is ~0.75%. These death rates seem plausible for extremely dense areas (NYC is something like 0.25% or so, with pretty aggressive action, though taken late), but not really for entire nations on the scale of UK or US.
And a more than order of magnitude difference based purely on national-level government action seems questionable, since at least in the US it seems that state-level government actions are poor predictors of “on-the-ground” individual behaviors. Maybe UK people trust/follow their government more, but…
There’s reasonably good evidence that the lockdown numbers that were predicted were too low because a low value for R (2.4) was used by the Ferguson. This led to overoptimism on the part of the team, and with other scientific advice combined with the political stance of the UK government led to a delay of a couple of weeks in implementing full lockdown. If they’d been aggressive and implemented lockdown earlier deaths would probably be about half of the current value.
The US never implemented lockdown. NY did after NYC dallied. CA moved first, and the Bay area before the state (LA county dallied and the numbers reflect that). But even our lockdown in CA wasn’t all that stringent and after about four weeks began to be ignored by many, with very little enforcement.
I see nothing to make one think that the predictions for total deaths in the UK/US in the absence of mitigation action was too high. However, the Ferguson team made clear that no action wasn’t really a possibility, human nature is such that people will modify their behavior to some degree without government forcing it. We saw this in the Bay area of CA when companies began asking people to work at home before the six counties implemented their shelter-in-place directive, and other changes in behavior were happening, for instance.
Since distancing and masking appear to reduce R, there is an interesting thing I haven’t really seen discussed, and that this lowers the percentage of infection required to reach “herd immunity”, even if R isn’t moved below one. Of course, that only works if these actions continue as the peak of infections is passed, but these are mild measures compared to shelter-in-place and business shutdowns.
>>I see nothing to make one think that the predictions for total deaths in the UK/US in the absence of mitigation action was too high.
>>However, the Ferguson team made clear that no action wasn’t really a possibility
>>There’s reasonably good evidence that the lockdown numbers that were predicted were too low because a low value for R (2.4) was used by the Ferguson
I dunno. It seems like evidence keeps popping up suggesting that the virus was “loose” (undetected community spread) earlier than expected. Wouldn’t that suggest a rather lower R? (With a given number of deaths in April, an earlier start would seem to require a slower spread.)
Couldn’t the too-optimistic lockdown predictions instead be because people don’t adhere to lockdowns very well?
>>The US never implemented lockdown.
I agree there, US as a whole did not; some states and cities did, some did a weak version, some didn’t lock down at all.
>>I see nothing to make one think that the predictions for total deaths in the UK/US in the absence of mitigation action was too high.
I kind of do. As you said, our mitigation was not very good, and I don’t think the US will see anything even close to 1.1 million deaths.
Although that also depends on how long one expects this to last, and how seasonal one expects it to be.
We are at 120k deaths in something like 4 months. Death reporting lags, so let’s say it’s actually 130k.
For the US to have more than, say, 330k deaths (0.1%) would mean that either the death rate increased sharply again*, or the pandemic goes on and on (ie no vaccine this spring).
I am pretty optimistic about a vaccine this spring (maybe even this winter).
*The 7-day average is 500-something deaths per day and dropping right now… but again, reporting lags, and death lags infection. I wouldn’t be surprised to see some uptick from the Southwest, but I *would* be surprised to see anything like late-April levels (over 2000/day) again.
In some states, confirmed cases are rising but deaths are falling; in at least a few cases, this has been going on long enough that lag alone can’t explain it.
>>However, the Ferguson team made clear that no action wasn’t really a possibility,
Yeah, it’s more the ~0.37% (250k deaths for UK) that I am questioning – I agree the ~0.75% was a hypothetical situation which couldn’t actually happen in practice.
I don’t think any nation on Earth will see anything like 0.37% of its population die of COVID, certainly not any nation with a population greater than, say, 1 million. Generally those nations with worse health systems tend also to have younger populations.
confused: I think a thing you need to be careful about when considering the effect of heavy mitigation / NPIs is whether they are the reason we have lower death rates.
Specifically, when the virus is very virulent, it tends to send its host to the hospital and/or kill it off. The result is it’s usually hard to spread a virulent strain except at hospitals.
When everyone outside a hospital is doing lots of NPI: distancing, masks, staying home, etc. Then there’s an enormous selective pressure towards the virus becoming *less virulent* and *more contagious*.
I think there are indications now that we may have a virus that’s far less severe than it was back in March in Italy/Spain/NYC. But that wouldn’t necessarily have happened without all the selective pressure. The NPIs may have saved people not only by slowing infections, reducing hospital load, giving time for people to learn how to treat the virus, giving time for people to learn how to keep it out of nursing homes and other places, giving time to ramp up testing and case contact tracing etc… But ALSO because the virus we have now is less virulent and specifically because everyone stayed home and made it hard for the virus to spread.
Anonymous
“>>I see nothing to make one think that the predictions for total deaths in the UK/US in the absence of mitigation action was too high.
>>However, the Ferguson team made clear that no action wasn’t really a possibility”
Your point?
@dhogaza: That “Anonymous” was a mistaken incomplete version of my comment immediately below.
@Daniel Lakeland: maaaybe. But coronaviruses don’t mutate as fast as influenza viruses, from what I’ve read, and the mutations that have been found so far are probably not terribly significant.
I think the apparent weakening is probably some combination of…
– improved treatments
– younger people being infected (lower risk, probably higher acceptance of risk, tiring of social distancing faster)
– higher proportion of asymptomatic and very-mild cases being detected.
On the third point, there is some uncertainty around accuracy of serological testing, and there is also (very tentative) evidence that some people may clear the virus without noticeable symptoms and without developing measurable antibodies. So the IFR may have been lower all along than we think.
Also, the ‘lockdowns caused weakening’ idea would suggest that the virus would be far worse in other parts of the world where a “pre-weakening” strain was present. (When did it arrive in Brazil or Mexico? Probably before the US had been locked down very much…) So I’m not sure it would really change the idea that if the model was correct, *some* nation would eventually see fatality rates on the order of 0.3%-0.4% of total population.
As bad as it is in Brazil, I don’t really think they are on track to 600,000-800,000 deaths.
I don’t see anything to suggest 0.37% is unreasonable. R0 of 2.5 yields herd immunity at 60%, and overshoot could add another 30% depending on what things look like when you get there. So 90% prevalence and 0.4% IFR looks on the underestimating side to me, just like 20k was.
My prior for how reality would’ve played out in other scenarios has to be informed by how it did play out under the one scenario followed. I don’t see anything in your comment that supports the idea they overestimated in one and underestimated on the others.
I think the best argument though is that we’re comparing apples and oranges between the two scenarios. The suppression scenario is highly dependent on minor timing differences — when going from an unmitigated epidemic that had a doubling time of 3 or 4 days to lockdown, it’s not hard at all to misestimate the timing and end up with two or even ten times the total infection count you expected, yielding the same multiple to deaths.
And all that said, nothing you’ve raised here contradicts my original point, which was that you didn’t have to have special insight into how nursing homes or multigenerational households work to realize that you’d likely fail at selectively protecting the elderly in a case where infection levels are high — you just had to listen to the experts who told you that. That Sweden chose to ignore that advice means they don’t get to absolve themselves by saying “our rates would’ve been much lower if we’d just selectively protected the elderly”. You weren’t gonna, and you should’ve known you weren’t gonna. Norway and Finland didn’t do succeed it at either; they protected their elderly the only way reasonably available — by limiting the infection rate across the population.
I think it’s implausible because I think 90% prevalence is very implausible (over a nation- or US state-sized area; maybe in a prison or something… though I think even they are more like 60-70%).
Has any epidemic/pandemic/outbreak, ever, gone to 90% prevalence in ~a year? Maybe measles but the R0 value for that is really sky-high, like over 10. Flu pandemics have been more like 30%-ish.
The R0 in most places is likely not as high as estimated for early hotspots like Wuhan/Lombardy/NYC with very high density compared to Sweden or the non-Northeastern US.
Also, COVID is super-spreader dependent compared to flu, which may lower the herd immunity threshold (due to network heterogeneity, but I don’t know much about this).
>>And often people who are making that argument don’t realize how many older people can’t realistically isolate because they have to work, go shopping, go to the doctor, take public transportation to get around, etc
>>Adding to the problem is that there are millions of grandparents acting as the primary caregiver for their grandchildren in this country
I think part of the issue is where you are drawing the line for ‘older’. There may be a bit of a false dichotomy thing. Once people start talking about 40%+ of the US deaths, and the majority in certain states, being in nursing homes, and the median age at death in various places being 80+ … but the population doesn’t divide into ‘young and healthy’ and ‘extremely old and frail’.
People in their 60s are at a lot higher risk than younger people but are much more likely to still be in the workforce, acting as caregivers, etc. than older people.
You can look at all-causes mortality on the EuroMomo website to see that Sweden is among the few European countries who haven’t managed to get their deaths down to baseline by now. Dead is dead everywhere, that compares unambiguously.
> Most in retirement homes tend not to be actively circulating in the general population.
Approximately the people in a retirement home on any given day are the staff.
The nature of close living in a retirement home means that once you have 1 infection, you likely have an outbreak before you discover it, so the efforts to mitigate the probability to get an infection in (like prohibiting visits by relatives, PPE for staff, etc.) are balanced by a bigger effect once the improbable happens. And general population prevalence is a factor in this.
Ultimately, Sweden seems to run a “flatten the curve”approach which does protect their hospitals successfully. If they did manage to get 20% of the population infected in 2 months, they might have population immunity by the end of the year, and then we’re going to have to wait until the epidemic is over for everyone else to compare.
They’ll not do well if it turns out industrialized countries can contain the virus using contact tracing. New Zealand did it, among others; Germany is up to ~150/401 counties (it fluctuates) with 0 cases over the last week amid a general reopening.
I imagine the infections like sparks running through the social network of society, with many flickering out; and once in a while a spark hits a node which explodes in a shower of new sparks, and fire-fighting tracers rush in to isolate/extinguish that cluster before the sparks can spread further. Containment depends on:
a) single-spark transmission R needs to be below 1 on average
b) cluster containment and isolation needs to be near perfect
c) cluster size needs to be small
Points b and c together determine how much a cluster amplifies the spread.
Some German regulations are focused on balancing b) and c): as restaurants open, they are required to log patrons’ phone numbers, so that if a pre-symptomatic person dines out, these contacts can be traced. Similar requirements apply to religious services, (small) events, hairdressers etc.
Correction:
Approximately *half* the people in a retirement home on any given day are the staff, *who are “general population”.*
>>I didn’t think it could happen, but now I think it’s starting to look like Sweden may eventually have more per capita deaths than Italy (they already passed France).
I agree, they probably will pass Italy.
But IIRC what the people favoring Sweden’s strategy were saying 2 months ago was that everyone will ultimately have about the same per capita deaths *after a year or so*, Sweden will just get there sooner with less economic harm (and be at herd immunity before a potential fall second wave).
We won’t really be able to tell whose strategy was best until we see whether Italy and other ‘lockdown strategy’ nations get a bad fall second wave.
Since we’re not seeing a dramatic summer drop in the US, a strong fall effect doesn’t seem to me to be as likely as it seemed 2 months ago (on the other hand air conditioning may mess with this — but flu is still seasonal in the southern US so…)
> Sweden will just get there sooner with less economic harm
Maybe. However, the expected GDP decline for Sweden is higher than for Norway or Denmark: https://oecd.github.io/EO-Outlook_chart_3/
I agree – and I am not saying Sweden’s strategy was right.
I am just saying that the arguments for that strategy can’t actually be falsified (or demonstrated to be true either) until we see what happens in the fall.
This would affect the economic arguments too — if Norway and Denmark suffer a severe second wave in the fall, but Sweden doesn’t (because they already hit herd immunity), that would presumably change the relative economic picture.
The arguments in favor of Sweden’s strategy were looking at results over the course of the whole pandemic.
Another thought – even if Sweden ends up with more deaths per capita than other European countries, I think it’s still significant (in terms of evidence about what the virus is actually doing) that they didn’t see the hospital overload that was widely predicted for such limited measures. I think *that* at least would be visible by now.
Is that because Sweden’s demographics are just *that* different from US/UK? Enough that an 8x overload becomes no overload?
Or is the R0 actually less than we thought, because the virus was spreading earlier than we thought?
Or have a lot more people been infected than we think, and thus a much smaller proportion of infected people are hospitalized? (NYC antibody results seem to rule that out, but I am not sure how solid that is — NYC is an outlier, serology test accuracy is apparently often questionable at least back in late April/early May, and we don’t know that all asymptomatic or very-mild infections produce antibodies at all.)
confused –
> Another thought – even if Sweden ends up with more deaths per capita than other European countries, I think it’s still significant (in terms of evidence about what the virus is actually doing) that they didn’t see the hospital overload that was widely predicted for such limited measures.
Obviously, the degree of hospital overloading would be contingent on a variety of factors specific to a given locality. Perhaps part of the reason they never switched from no SIPs to SIPs as the UK did, is because they had a medical care infrastructure that was robust enough to prevent overloading.
> Is that because Sweden’s demographics are just *that* different from US/UK? Enough that an 8x overload becomes no overload?
Obviously, it’s not just demographics, although that’s a factor (depends on what you mean by demographics to some extent. Do you mean that they have a high standard of living, do you mean the fact that they have an unusually high prevalence of single-person households, that the population density is low, etc.?) It’s also that they have a generally good healthcare system, that they have a robust social safety net that allows people to have a lot of work leave and to get other relevant supports. What is their hospital capacity? ICU bed capacity? Etc. All of those factors (and I’m sure others I missed) would be relevant context regarding the likelihood of hospital overload.
>>Obviously, it’s not just demographics, although that’s a factor (depends on what you mean by demographics to some extent.
I was thinking mostly of single-person households/low density, though lower obesity prevalence (than US anyway – no idea about UK) might reduce the proportion of total infections hospitalized. Sweden might also be better at preventive care, so other pre-existing conditions might be less common.
I think Sweden’s median age is a bit higher than the US’s, but within the range of US states.
These things probably overall benefit Sweden relative to the US, but I can’t see them being enough to convert the huge nearly-order-of-magnitude overload predicted by the Imperial College model into no overload.
Healthcare system though… I think US ICU capacity per capita is actually much higher than most European nations. We say European healthcare systems are better, but “better” has multiple dimensions; “more equitable” doesn’t necessarily translate to “better able to deal with a sudden large surge in demand”. The US also is large and was hit at different times; lots of resources were moved to NYC for example (hospital ship, lots of healthcare workers flew in, etc.)
So I’d be quite surprised if – taking moving resources around the US into account – Sweden was actually in a better place beforehand in terms of resources.
confused –
> These things probably overall benefit Sweden relative to the US, but I can’t see them being enough to convert the huge nearly-order-of-magnitude overload predicted by the Imperial College model into no overload.
The IC predicted a huge hospital overload for Sweden? Gotta link?
> … I think US ICU capacity per capita is actually much higher than most European nations. We say European healthcare systems are better, but “better” has multiple dimensions; “more equitable” doesn’t necessarily translate to “better able to deal with a sudden large surge in demand”
A quick Google tells me that the US has more critical care beds per capita than other counties, but less (far less than Sweden) hospital beds and doctors
Plus, Sweden surged capacity (I assume the extra capacity it wasn’t utilized).
>>The IC predicted a huge hospital overload for Sweden? Gotta link?
No, it predicted a huge overload for the UK and the US.
I’m saying that the differences between Sweden and UK/US seem likely to benefit them somewhat, but don’t seem nearly enough to account for a basically order-of-magnitude difference.
Surge capacity, sure, but presumably the Imperial College model took that into account for US/UK as well. (Without accounting for basic things like that, it would be kind of useless to even talk about hospital capacity, IMO.)
confused –
> I’m saying that the differences between Sweden and UK/US seem likely to benefit them somewhat, but don’t seem nearly enough to account for a basically order-of-magnitude difference.
I disagree strongly. Conditional projections of overload in US don’t apply to Sweden at all, IMO. The conditions, capacities, demographics, public attitudes, population density, etc. are all extremely different.
> Surge capacity, sure, but presumably the Imperial College model took that into account for US/UK as well. (Without accounting for basic things like that, it would be kind of useless to even talk about hospital capacity, IMO.)
Don’t know about IC specifically, but one of the criticisms of the modeling is that it assumed hospital capacity was static.
>>I disagree strongly. Conditional projections of overload in US don’t apply to Sweden at all, IMO
Possible. You could be right. But an order of magnitude difference still seems really huge.
Many US states are at a roughly Sweden-like level of “openness” (schools aren’t open, but they wouldn’t really be in session in late June anyway). Hospital capacity is starting to look frightening in Arizona and possibly Texas, which are relatively open*. In a few weeks to a month we will probably know one way or another… I really don’t think Arizona and Texas will implement stay-at-home orders again, and (at least in Texas, where I live) I don’t think they would be usefully followed even if officially implemented.
*Though not the most ‘open’ states.
>>Don’t know about IC specifically, but one of the criticisms of the modeling is that it assumed hospital capacity was static.
Yeah, true.
Even there I think there are two levels of “static”. There’s normal capacity, and there’s “surge” capacity on the hospital/hospital system level. But then there’s also adding capacity by more extraordinary means like sending a Navy hospital ship to New York City.
I think that excluding “extraordinary” capacity increases would make the modeling inaccurate, but might be justifiable since we might not really know how much “extraordinary” capacity we can provide until we actually have to do it. (People may find solutions during a crisis that wouldn’t have been thought of before, or might have been considered “not good enough” absent the pressure of a crisis.)
But excluding ‘normal’ surge capacity would just be wrong.
confused –
> But IIRC what the people favoring Sweden’s strategy were saying 2 months ago was that everyone will ultimately have about the same per capita deaths *after a year or so*, Sweden will just get there sooner with less economic harm (and be at herd immunity before a potential fall second wave).
Yes. That is what many argued. Of course, most who made that argument made huge assumptions about the economic advantages of Sweden’s approach – almost always in association with their political/ideological orientation. What’s interesting is that many were quite sure despite lacking supporting evidence. The assumption was made that since there were “costs” associated with SIP orders, those cost would necessarily be a differential cost relative to not issuing SIP orders.
In fact, it isn’t clear that there will be a significant differentially beneficial economic effect from Sweden’s approach. And as we go forward it only gets more complicated for a while before becoming easier to reach a solid conclusion. We have to see what happens with “re-opening” in places like Denmark, Norway, and Sweden. Are they able to better open up because the spread is under better control? And what if there is a widely distributed vaccine on a relatively short time frame? In that case, the relative merits of fast/deep vs. slow/shallow can change diametrically. More deaths (more quickly) would then be a differential negative outcome in Sweden if a vaccine is distributed, as opposed to a scenario where no vaccine is developed and in the end a similar % get infected regardless. What is the economic “cost” of a life needlessly lost?
> We won’t really be able to tell whose strategy was best until we see whether Italy and other ‘lockdown strategy’ nations get a bad fall second wave.
Italy and other countries are a bad basis of comparison without much higher quality data than what we have. The conditions in Italy were vastly different than in Sweden. Part of the reason why they took different approaches is because those starting conditions were vastly different, and because they were fundamentally differently positioned to implement different policies. For example, average age is much higher in Italy. Italians live in much more densely packed communities and are much more likely to live in intergenerational households. Sweden was much better situated for people to work at home. Swedes tend to live in single-person households, let alone one- or two-generation households as opposed to three-generation households. Italy sustained a much higher rate of travel to/from China. On the other side of the coin it appears that in Sweden they are not providing oxygen therapy to infected seniors in nursing homes. Is that a factor in the higher death rates?
In the end, people are very anxious to use Sweden as a way to prove their political ideology correct. It’s very unfortunate.
> Since we’re not seeing a dramatic summer drop in the US, a strong fall effect doesn’t seem to me to be as likely as it seemed 2 months ago (on the other hand air conditioning may mess with this — but flu is still seasonal in the southern US so…)
Seems to me that many people are much too quick to draw conclusions. For example, there was great deal of speculation about a seasonal effect in the US that doesn’t seem to have materialized – but even there, it’s still too early to really tell.
And I’ll also note that in order to really understand the causal mechanisms, a sensitivity analysis needs to be done of the different interventions. Closing high schools and colleges, and limiting large gatherings, and having people work at home all might be much more explanatory than other interventions. Or they might not be. But the point is that those interventions all took place in Sweden as well as in countries with SIPs. As such, assumptions about the causal impact of Sweden’s approach versus approaches in other countries are useless unless they control for the impact of those variables.
There’s just so much about this issue that’s vastly complicated – yet so many people are very quick to draw conclusions. Seems to me like just another political proxy that people use mostly for bias confirmation.
>>Of course, most who made that argument made huge assumptions about the economic advantages of Sweden’s approach
Yes; I think there was insufficient attention to how interconnected the economy is – one nation’s economy is affected by what happens in others. And people will be less willing to go to restaurants etc. even if they are open.
>>In fact, it isn’t clear that there will be a significant differentially beneficial economic effect from Sweden’s approach. And as we go forward it only gets more complicated for a while before becoming easier to reach a solid conclusion.
Exactly. It isn’t and can’t be clear. You can’t judge a strategy that is aiming for better overall results 12+ months down the road 3 months in.
I don’t think we can make any confident statements until next year.
>> And what if there is a widely distributed vaccine on a relatively short time frame? In that case, the relative merits of fast/deep vs. slow/shallow can change diametrically.
Absolutely.
>>What is the economic “cost” of a life needlessly lost?
That’s a very fraught question. You can use the value of a statistical life type approaches of course.
But I don’t think it’s really necessary here. As I understand it, the argument was that Sweden would see roughly the same deaths AND less economic harm (after the whole pandemic). That can be evaluated without weighing lives vs. economy.
>>Italy and other countries are a bad basis of comparison without much higher quality data than what we have.
Yes, that’s true also.
>>Seems to me that many people are much too quick to draw conclusions. For example, there was great deal of speculation about a seasonal effect in the US that doesn’t seem to have materialized – but even there, it’s still too early to really tell.
I agree. I think we can fairly confidently say that at least in the US it’s less seasonal than ordinary seasonal flu, but that doesn’t mean no seasonal effect. And we really don’t know how many infections there were in Feb/Mar/Apr.
There are some states in the US where “confirmed cases” are rising but hospitalizations and/or deaths are not (reporting for hospitalizations is however inconsistent). In at least some of these, that ‘divergence’ has lasted long enough that infection-to-death lag alone doesn’t seem to be a valid explanation (Georgia seems to have diverged at least 6 weeks ago). So there might have been a much higher ‘seasonal’ peak in spring not detected.
confused:
“Exactly. It isn’t and can’t be clear. You can’t judge a strategy that is aiming for better overall results 12+ months down the road 3 months in.”
You can judge a strategy that claimed Sweden might reach herd immunity levels in May a month after May has passed, though … the strategy most emphatically wasn’t a 12+ month strategy.
What I meant by the 12+ months is the idea that countries that locked down and thus limited infection rates would see a bad second wave at some point, thus reaching herd immunity eventually anyway.
So Sweden having a higher death rate than another European nation in June or July doesn’t necessarily mean their strategy was worse overall, that can’t really be decided until we have time to see whether a fall second wave happens or not.
As for herd immunity in May — infections don’t go to zero immediately upon reaching herd immunity. And we don’t know either the herd immunity threshold in Sweden (probably will not be the same everywhere due to contact networks) or the true infection rate in Sweden (how good are their serology tests? Do some people, especially younger, clear the infection without producing detectable levels of antibodies – via innate immune system or T-cells?)
I agree that Sweden probably did not reach herd immunity by the end of May, but being 1 month off is not that terrible as far as modeling goes. I won’t be ready to say their predictions were radically wrong until late August (because if herd immunity was reached today, the decline in R might not be immediately obvious, due to lags from infection to death and lags in reporting).
“As for herd immunity in May — infections don’t go to zero immediately upon reaching herd immunity.”
Now you’re grasping at straws. No, they don’t go to zero immediately, but they start declining quite quickly. And that didn’t happen. And the Swedish authorities admitted they’d made a bit of a good in their calculations. And are no longer attempting to predict when herd immunity might be reached. Get real, please – if there were any real straws to grasp at the leadership of the country would be doing so.
>>Now you’re grasping at straws
Not really, I don’t have anything invested in the Swedish approach. But I just don’t think there is as much certainty as you are implying.
>> No, they don’t go to zero immediately, but they start declining quite quickly.
Herd immunity just means R has fallen under 1 due to the lack of susceptible individuals, doesn’t it? If R is somewhat below 1 but not by *that* much, why couldn’t there be a slow decline?
>> And that didn’t happen.
I am not sure anyone, even the Swedish authorities, has a decent idea of what the infection rate in Sweden is. (Their testing seems quite poor, as the observed CFR is implausibly high. So daily new cases are probably practically meaningless.)
The death rate seems to have been declining for a while. I don’t see why the data is necessarily incompatible with R having been under 1 for a while.
“The death rate seems to have been declining for a while.”
Sweden has made it clear that they screwed up in their attempts to keep it out of long-term care facilities, and burned through a bunch of deaths of these extremely vulnerable people as a result. Despite focusing on the protection of the most vulnerable people as being an important part of their strategy.
Since then they claim to have gotten that situation under control, with a subsequent lowering of the death rate overall.
Under these circumstances, I don’t see that the declining death rate tells us much about R. Just IMO.
I have seen recently that part of the issue with the high death rate in LTCFs in Sweden is due, to some extent, with their casual attitude towards treating infected older people, i.e., not treating them with relatively uncomplicated oxygen therapy. So that could have nothing to do with the effectiveness of their policies regarding spread, per se.
That said, I never thought that their death rate would go above that of France. Not only has it done so, but it’s about to overtake Italy and may even go higher than in Spain or the UK. Yikes.
Seems to me that there a very long list of reasons why Sweden’s rate should be lower relative to those countries. And the rates relative to other Scandanavian counties also strongly suggests that those who claim that government interventions don’t have any effect on reducing spread – at least over the short term – are clearly blinded by ideological biases.
Consider how Switzerland at one point had a relatively similar death rate – presumably for reasons like lifestyle predictors of greater spread and proximity to Lombardy and amoint of travel to/from hotspots – and now the death rate there is less than 1/2 that of Sweden.
We need to wait to evaluate the long term scenario, in terms of economic and health outcomes. But I can’t see any reasonable argument that Sweden’s outcomes are consistent with a view that government mandated social interventions don’t have a significant impact on rate of spread (and associated # of deaths, even if that isn’t necessarily directly proportional).
Maybe Sweden is an outlier for some reason with respect to a typical causality between SIP orders and health outcomes – but I haven’t seen an argument that convinces me that is the case. If someone wants to argue that SIP orders are totalitarian, that’s obviously a matter of personal priorities: A whole other category of debate
>>I can’t see any reasonable argument that Sweden’s outcomes are consistent with a view that government mandated social interventions don’t have a significant impact on rate of spread
I agree with this. I’m just saying that if hospitals are never overwhelmed (which they haven’t been in Sweden, and probably won’t be) “rate of spread” will not necessarily correlate with “total deaths over the course of the pandemic”.
Obviously if you eradicate the virus completely total deaths will be lower. But within the range between “eradication” and “overwhelming hospitals”, rate of spread will only affect total deaths if a vaccine can be widely distributed before the pandemic burns out naturally.
(Which I am personally pretty optimistic about, but it is far from certain, so IMO still too early to call Sweden’s strategy a failure. Though it definitely looks a lot worse than it did a month ago.)
Sweden doesnt look exceptional at all to me: https://www.euromomo.eu/graphs-and-maps/
>>Under these circumstances, I don’t see that the declining death rate tells us much about R. Just IMO.
That’s entirely possible! Maybe even more likely than the alternative.
On the other hand, lag in reporting of deaths may make a decline look slower (current deaths look higher and deaths at peak look lower) than it actually is. This seems to have happened and to be happening in some US states; I am not sure what Sweden’s reporting system is like.
I am just saying I don’t think the information available to us is good enough to draw any strong conclusions one way or another. (Given infection-to-death lag plus lag in reporting of deaths, hitting herd immunity might not be obvious for a month or more after the fact, unless testing remained consistent throughout.)
Anoneuoid –
> Sweden doesnt look exceptional at all to me…
It has a much higher death rate, and far more infections (to the extent that we can tell without really having a good control on testing), than the countries that are the most similar in many important factors.
It has many structural advantages compared to those countries that have a more similar death rate and infections rate, and after the initial stage of the pandemic, it has trended far worse relative to practically all countries outside of maybe a few other countries that also trended relatively poor, like Brazil and the U.S.
And you’ve also, effectively, cherry-picked, You ignored a whole slew of countries, the vast majority in fact, that have fared better than Sweden. Presumably you did so because there are important commonalities among countries in Europe – but you effectively ignored any ranking among those countries on the basis of similarities. If you’re going to use commonalities as exclusion criteria for your comparison, you should be consistent.
Sweden has fared far worse than the other Scandinavian countries, those countries which are the most similar. They have fared far worse after the initial stages than other countries in Europe which didn’t have certain advantages that Sweden had in the beginning (i.e., proximity to Lombardy, % of people who live in single-person households, ability to take leave from work, ability to work from home, low population density, travel to/from China, % of multi-generational households, # of infections before community spread was discovered, access to healthcare, reach of social programs network, etc.).
Do you disagree that Sweden had structural advantages over the other countries that rank similarly in terms of deaths per capita? Do you think that there were also structural disadvantages in Sweden? The only one I can think of is their apparent casual policy on treating infected elderly patients (which if true, I think is a fairly significant factor). If you think what happened there is unexceptional, how do you describe the dramatically different trend line in Sweden as compared to a country like Switzerland?
Can someone explain to me why some comments just go missing at this blog – not even with a message that they have gone into moderation (and which later sometimes get posted)?
Anoneioud –
> Sweden doesnt look exceptional at all to me:
I think that Sweden had certain structural advantages over the countries that have a similar death and infection rate. The countries that are the most similar, with similar structural advantages, have fared considerably better on health outcome measures.
Those countries that didn’t share the structural advantages, on the whole, started out much worse relative to Sweden in terms of outcomes, but Sweden has trended much worse than them after starting out at an elevated level. Sweden started out at an elevated level due to reasons that had nothing to do with policy choices. If we’re just judging by association with policy choices, it looks like Sweden has trended much worse than those countries which have similar outcomes at this point.
If you think what happened there is unexceptional, how do you explain the dramatically different trend line in Sweden as compared to a country like Switzerland? Do you think that there isn’t really a long list of structural advantages that Sweden had going in to the pandemic, relative to those countries which had similar outcomes at this point? I’ll list some that I think are important: Proximity to the hotspot of Lombardy (and presumably levels of travel to/from Lombardy), I’m guessing level of travel to/from China, population density (and % who live in rural communities at least in comparison to some of the other European countries), % of people who live in single-person households, % of people who do not live in multi-generational households, ability to work from home, level of social safety net support, ability to take paid leave or vacation time…I would guess maybe a lower level of comorbidities, I would guess a higher baseline health status and better overall health and lifestyle behaviors.
I would guess there are more. I would guess that there might be some structural disadvantages for Sweden relative to health outcomes from the pandemic; maybe average age – which is important. Or maybe number of older people living in LTCFs. But I can’t think of any others. The closest I can think of as a policy outcome, would be if it is indeed true that they have taken a more casual approach towards medically treating infected seniors.
I notice that you picked European countries as a comparison, not including the vast majority of countries around the world which have fared better than Sweden in terms of health outcomes. Presumably you did so because there are more cultural or economic or political commonalities with the countries in Europe. But you didn’t rank countries within Europe with respect to the extent of those commonalities. Why not? I think that if you did, Sweden would look like an outlier.
I have had quite a few comments just fail to appear – with no message about them going into moderation. Sometimes they later show up as posted, and sometimes mot.
Does anyone else have that happen? If so, can you think of any reasons why it happens? I assume something gets caught in the spam filter – but sometimes when that happens I get a moderation message. What causes the different kinds of situations? Just happened twice, the second time after I rewrote the basic comment but it clearly wasn’t the same. Any tips as to what comments get thrown into moderation (there were no links)?
@Joshua
Euromomo reports data from whatever countries participate in that project. I didnt choose the comparison.
But others are saying it looks exceptionally bad on here and I dunno what data they are looking at or how it was arrived at.
You can also look at Belarus, where the president said its cured by playing hockey, etc and keeping your blood flowing. Ive also heard anecdotaly from people tested positive that they felt much better when forcing themselves to move around instead of lay in bed. Could make sense if a major problem has to do with blood clots and endothelial dysfunction.
I mentioned earlier that pilates was invented to fight the “spanish flu”, which shared many symptoms.
So I dunno, all this data is messy as can be.
As to avoiding the spam filter. Add an email address when you post, dont post many times in quick succession, and dont include more than one link.
“The infection fatality rate of COVID-19 in Stockholm – Technical report.”
“Our point estimate of the infection fatality rate is 0.6%, with a 95% confidence interval of 0.4–1.1%. For the age group 0–69 years, we get an estimate of 0.1% (c.i. 0.1–0.2%), and for those of age 70 years or older our estimate is 4.3% (c.i. 2.7–7.7%).“
https://www.folkhalsomyndigheten.se/contentassets/53c0dc391be54f5d959ead9131edb771/infection-fatality-rate-covid-19-stockholm-technical-report.pdf
Interesting.
I’m kind of surprised by the 0.1% for the population under 70. That seems quite low.
Why group together all ages 0 – 69? That large an age span doesn’t make sense to me.
Probably because the number of fatalities under age 69 is relatively small, so they’re trying to get large counts to reduce the naive statistical error estimates… Bayes would help a lot I think, and treating this as a regression (an IFR curve as a function of age).
The give also a more detailed break-down:
Age 0–49 0.01% [0.00 0.02]
Age 50–59 0.27% [0.15 0.50]
Age 60-69 0.45% [0.25 0.88]
Age 70-79 1.95% [1.16 3.40]
Age 80-89 7.20% [4.54 12.84]
Age 90+ 16.21% [10.11 29.50]
OK, wow.
I wonder if these can be right? 0.6% overall for Sweden does not seem too low – Iceland (with an admittedly small sample size – 10 deaths) saw a CFR of 0.55% Iceland tested a huge proportion of their population, but they might still have missed some asymptomatics, so the IFR could even be a bit lower.
But 0.01% for under-50 is really low. Isn’t that less than the risk for this age group with 2009 H1N1 (Which was about 0.02% populationwide, but pretty flat with age, maybe even a bit worse for the young)?
> 2009 H1N1 – Which was about 0.02% populationwide
This suggests that IFR was quite lower than that, in the range 0.001%-0.01% : https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3809029/
“In 14% (11/77) of the case fatality risk estimates, the denominator was based on an estimated number of infections. Among those 11 studies, 8 used denominators based on population serological studies, while the others used modelling or multiplier approaches. Those risks tended to remain stable over time, although no such estimates were published within the first year of the pandemic (Figure 3). Estimates ranged from 1 to 10 deaths per 100,000 infections, with substantial heterogeneity [I2=94.46%].”
The lower part of that range is impossible, and even the upper part seems far too low.
CDC estimates ~12,500 deaths in the US. https://www.cdc.gov/flu/pandemic-resources/2009-h1n1-pandemic.html
The US population at the time was 308 million, so ~0.004% of the US population died. I don’t think that 40% of the US population was infected, so even 0.01% seems implausibly low.
Related to cross-cultural estimating of fatality rate, a disturbing article:
https://www.cgdev.org/blog/predicting-covid-19-infection-fatality-rates-around-world
Disturbing — if believable. But this doesn’t sound remotely believable.
“To gauge how much fatality rates might vary with health system capacity, we draw on estimates of the infection fatality rate for another viral respiratory infection, namely influenza. We focus on children under five years old,”
Um, what??? Influenza is much more dangerous than COVID in <5 years old. They are extrapolating from influenza to COVID and drawing from a demographic where influenza is utterly unlike COVID (and we don't even really know why COVID acts this way, it is certainly atypical of viral respiratory infections).
They might turn out to be right in the sense of "higher than expected deaths in the developing world". But this argument is still very poor.
But the "developing world" includes radically different situations. Those with very high HIV/AIDS prevalence like much of southern Africa, or those with limited healthcare capacity but median ages that aren't all *that* low by developing-world standards*, might see high IFRs.
*Brazil might be in this category, I don't know anything about their healthcare system but their median age of ~33 is pretty high for Latin America.
confused –
Seems to me they didn’t extrapolate directly from influenza case fatality, but based on fatality rates resulting from “seasonal-influenza-precipitated acute lower respiratory infection (ALRI) amongst children aged 12-59 months” across different nations. ALRI – not influenza.
Which might not make sense if children developing ALRI from seasonal influenza in developing countries shouldn’t apply for children developing ALRI in developing countries from COVID.
The authors seem to have quite a bit of relevant expertise. Which doesn’t make them right, but it does suggest that they might not make an obvious analytical error as you suggest v
“Seasonal influenza precipitated”, so I don’t think that resolves the problem.
>>The authors seem to have quite a bit of relevant expertise. Which doesn’t make them right, but it does suggest that they might not make an obvious analytical error as you suggest
One would think, but I’ve seen a lot of quite questionable things said by apparent experts over the last 3-4 months. I think it’s partly because of time pressure & the emotional weight/politicization of the issue, and partly (as in this case) because of applying lessons from past epidemics/pandemics that don’t apply to this specific disease.
COVID’s comparative lack of effect on the very young is extremely atypical. Any comparison which relies primarily on the youngest age groups, IMO, is useless from the start.
confused –
> COVID’s comparative lack of effect on the very young is extremely atypical.
Is it? Do you have a link?
Not a specific link off the top of my head, no, but tons of infectious diseases hit the very young/very old hardest. That’s why infant mortality is such a huge factor in total life expectancy without access to modern medicine.
Seasonal influenza tends to have an U-shaped death curve, with higher risk at the youngest ages, very low risk at most ages, and the most risk at the oldest ages.
Pandemic influenzas vary. 2009 flu had a fairly flat curve. 1918 flu had a triple-spiked curve rather than a U-shaped curve, with a spike in the 20s and 30s as well as youngest and oldest.
COVID is unusual because it is milder at the youngest ages than in younger adults in the prime of health, say 20s-30s. Not many things work like that. (I mean, polio was worse if you caught it later in childhood rather than immediately after birth. But still not worse for adults. And polio is fairly atypical too.)
confused –
> COVID is unusual because it is milder at the youngest ages than in younger adults in the prime of health, say 20s-30s.
I thought I’ve read differently – that the age profile of deaths is not atypical.
Although I also recall hearing that flu vaccines are particularly important for younger and older people. Hmmm.
A quick Google:
https://www.sciencedaily.com/releases/2018/02/180215165511.htm
https://www.scientificamerican.com/article/flu-shots-may-not-protect-the-elderly-or-the-very-young/
>>I thought I’ve read differently – that the age profile of deaths is not atypical.
What I’ve read is that the age profile of deaths is not atypical (corresponds roughly to the overall risk of all-causes death by age) *except at the youngest ages*.
Which are specifically the ages (<5) being discussed here.
Also, that statement was in context of US and Europe and maybe China – no good COVID data at that time (or maybe even now) from poorer nations. The all-cause death curve by age is quite different (much larger infant mortality in some poorer nations).
>>Which might not make sense if children developing ALRI from seasonal influenza in developing countries shouldn’t apply for children developing ALRI in developing countries from COVID.
Well, here’s the problem with that — very, very few in this age range develop serious respiratory issues from COVID. Few enough that it won’t have a detectable effect on the nation’s IFR.
But what they’re doing isn’t quite that bad. They are using fatality rates of influenza in the under-5 population as a measure of health system ability to deal with COVID.
But I don’t think this is valid. Influenza is long known and well understood; developed-world health systems are really good at dealing with it. COVID is new and poorly understood; we’re not very good at dealing with it. We are learning a lot more (better supportive care, remdesivir, dexamethasone) but given lags from infection to death and death to reporting, improvements in IFR haven’t really shown up clearly yet.
Since developed-world health systems are much less competent at dealing with COVID, the difference between developed-world and less-developed should be much smaller than with influenza.
(This also implies that if COVID is still around 5 years from now, its IFR in the developed world will be far lower.)
confused –
Take a look at page, 9-10 and see what you think.
confused –
And they spell out details for much of their methods for statistical adjustments in the appendices. Take a look and let me know what you think.
I read it. I’m still not convinced.
What I’m complaining about isn’t the statistical adjustments per se, but the starting assumptions. (“Garbage in, garbage out.”) If you start with data that has essentially no relevance to COVID, no amount of statistical adjustment will give you useful results.
I am sure that nations with worse health systems will see a higher IFR than nations with better health systems but otherwise similar demographics. I am just skeptical that the effect will be *that* large.
(Also, the before-adjusting-for-health-systems IFRs seem a bit high to me. Their lowest is 0.11%; I’d expect those Sub-Saharan African nations with super-low median ages and lower HIV prevalence to be lower than that. Singapore’s IFR is probably below 0.1%.)
Also, they comment that mortality under 5 is used (among other reasons) because this age group avoids issues with comorbidities.
This seems way wrong. Sure, this age group won’t have the comorbidities we are familiar with.
But infant/early childhood mortality is frighteningly high in the poorest nations due to conditions that are rare or trivial in the developed nations, malnutrition is common, etc.
There probably aren’t enough people with malaria or severe malnutrition in the US or Italy for those sorts of things to show up as comorbidities in the statistics. That doesn’t make them irrelevant.
Influenza is much more dangerous than COVID in this age group (specifically – definitely less dangerous overall!) If that vulnerability is exacerbated by these sorts of conditions, then any relevance vanishes.
Based on deaths per 100,000 using several types of regression models, the U.S. is on target to surpass Sweden in deaths per capita by year end 2020 — not even age adjusted for Sweden’s much higher proportion of 80+ year old citizens. We trashed our economy and took on trillions of debt and Sweden did not. I believe Sweden will ultimately be proven to have taken the wisest course of action when the first full year data is analyzed. Sequester the old and infirm, not the young and healthy. Keep everything open to the extent hospitals can handle the load. It is the ultimate death toll mitigation that is ultimately most important, not the shape of the curve, cases, etc. Sweden’s rip off the band aid quickly approach was better than our slow and painful band aid removal.
But the US did literally the worst job of any country in terms of actually taking any active action to mitigate anything.
On your band aid analogy it’s like Sweden decided to rip the band aid off so fast it takes huge quantities of skin, Germany decided that if they just didn’t keep cutting themselves with razor blades they didn’t need to worry about how to put band-aids on or off, and the USA is drunk and belligerent and taking bets on how deep it can cut itself and how much blood it can lose and still stagger home.
Worst of *any* country? What about Brazil etc.?
Comparing to Western Europe and the wealthier countries in Asia, sure.
The US response to crises is often poor early on (Great Depression, etc.) but we always muddle through and often come out stronger anyway. Poor centralized response is the inherent weakness of our strengths, IMO.
But for all that, I don’t think our actual per capita death rate will be the highest. Not sure we will pass Sweden – the shape of the death curves look very similar, and right now Sweden has more per capita deaths. (In both Sweden and the US confirmed cases are increasing but deaths are declining.) Passing Belgium seems very improbable. The situation in Houston, Phoenix, etc. looks bad, but seeing NYC/New Jersey-level deaths there is very unlikely, due to better medical knowledge and younger population infected.
The greater New York metro area *both* has an extremely high population and saw an extremely high death rate per capita. That’s very unlikely to be repeated elsewhere in the US.
I meant any country of similar level of development to Sweden. Sweden has $55k/capita GDP whereas Brazil has about $9k/capita
The US response has been absolutely terrible.
>>I meant any country of similar level of development to Sweden.
Yes, this I will agree with.
Although every other country with remotely comparable per-capita GDP is far smaller than the US in terms of population, and most have nothing like our degree of internal complexity (federal system with 50 states, huge rural/urban disparity, etc.)
>>The US response has been absolutely terrible.
Certainly.
But not, I think, really *surprisingly* so. (It was surprising to many people, but that is I think due to comparisons to nations with a more centralized structure, a much less individualistic culture, etc.)
The US didn’t handle HIV/AIDS’ arrival terribly well either, and the 2009-10 flu pandemic turned out to be far milder than feared. We just haven’t had to deal with anything like this in over 50 years – and even the 1957-58 and 1968-69 pandemics had little cultural impact (and relatively little action taken), certainly nothing like the level COVID has had. There are pandemic plans, but the failure of testing in Jan/Feb basically destroyed them all, and large bureaucracies are not good at adapting on the fly.
And the US’ *initial* response to a new crisis is often poor.
As much as I dislike the current administration, I don’t think the failures are that simple in origin. I think they were unfortunately very likely given the structure of CDC, FDA, etc. We could have gotten lucky with the testing, but…
> We trashed our economy and took on trillions of debt and Sweden did not.
The economic impact may not be that different: the OCDE forecasts 2020 GDP growth to be 7 percentage points lower in Sweden, 8 percentage points lower in the US.
> Keep everything open
I’m not sure that’s an accurate description of the situation is Sweden. Gatherings of more than 50 people were banned in March and there are restrictions in some activities (like bars and restaurants).
I think Sweden’s real advantage will be in less opportunity cost in things like missed education, and less social disruption overall. Things that will be very hard to measure but may be as significant (or more so) 5 or 10 years down the road as the effects of the pandemic itself. Historically pandemics don’t seem to leave as much economic or social damage as one would expect from the number of deaths (1957-58 and 1968-69 made little historical impact, and are forgotten by many of those who lived through them. Even the social and political impacts of the exceptionally deadly 1918-19 pandemic were far smaller than, for example, the Vietnam War or the Great Depression.)
Both the Vietnam War and the Great Depression were *symptoms* of a country with terrible policy. They were also causes of long term problems I agree, but they were both totally avoidable with better policy.
Sure, but I’m not talking about the causes of the events, but how deeply they are etched into the collective memory of the populace/society. Those might not have been the greatest examples, granted – things due to human stupidity are seen as ‘worse’ than natural disasters – but IMO it is pretty surprising that the 1968 pandemic killed 100,000 people in the US (out of a much smaller population) and before COVID most people didn’t even know it had happened. 1957 was worse and still didn’t make much of an impact.
1918-19 was incredibly lethal yet had very little social impact after it was over. Sure it was somewhat overshadowed by WWI… except that many countries weren’t really involved in WWI and the flu hit everywhere except a few remote islands.
Although, ultimately, this is what we would expect, I guess. Most of history has seen a far higher burden/risk from infectious disease — of course people and societies are capable of dealing with it without vast disruptions (except in the very worst plagues), or civilization wouldn’t have survived. IMO, COVID is largely so frightening/socially disruptive since we have done so well at eliminating other infectious diseases in the developed world.
MBA Statistician:
“We trashed our economy and took on trillions of debt and Sweden did not. I believe Sweden will ultimately be proven to have taken the wisest course of action when the first full year data is analyzed.”
Others have pointed out that Sweden’s economy has suffered, too.
But let us say that due to rash reopening in the US and our unwillingness to practice social distancing, masking, etc that we do indeed pass Sweden in terms of deaths per capita.
I wouldn’t use that as a base for declaring that Sweden has taken the wisest course of action, it would simply show that we’re being really stupid here in the US.
Compare Sweden with countries that have actually done an effective lockdown with much lower loss of life. Norway and Denmark, if you want to look at neighboring Scandanavian countries. Or Germany, as mentioned by Daniel Lakeland. Then explain to us why Sweden’s course looks “wisest” … as opposed to potentially merely less stupid than ours.
It feels like there’s a concerted effort by the media to declare the Swedish approach a failure. Every couple of days there is some new story about what went wrong.
But looking at their data (if Worldometers is accurate), their daily deaths apparently peaked back on April 8 and have been steadily declining since. In the past month they’ve reported very deaths. I remember reading predictions that Swedish deaths would surge this summer (as confirmed cases did continue to rise until June) but that hasn’t been the case at all.
Sweden still has a bad-looking number of deaths per million, but that appears to be mostly due to April and early May. At this point it seems that they are in largely the same position as other European countries. On July 17, for example, they reported 152 new cases and 10 new deaths.
We should be careful about drawing too many conclusions too soon about this pandemic, it is ongoing and we still may have a lot to learn.
John –
> It feels like there’s a concerted effort by the media to declare the Swedish approach a failure
Your frame of “the media” is too broad, imo. There is much by way of “the media” who are making a concerted effort to portray Sweden as a success story w/r/t policies to address the pandemic.
> At this point it seems that they are in largely the same position as other European countries.
Although the rate of increase in per capita death rate relative to European countries is starting to look lore similar, it was significantly higher up until very recently and even now is higher (i.e., theay well pass Italy on per capita death rate in a couple of weeks although it is lower there now).
It does seem to me that there is a push from both sides of the political aisle to spin Sweden”s outcomes to lifn up with ideological preferences. It’s an unfortunate manifestation of our underlying tribalism.
>
Posted too soon…
> We should be careful about drawing too many conclusions too soon about this pandemic, it is ongoing and we still may have a lot to learn.
No doubt – the wisdom, or lack thereof, of Sweden’s covid policies could well take on a different look over time. If it turns out that their economy takes a significantly smaller hit due to their policies relative to other countries, then that will change the lens to use for evaluating their choices – but as of yet they seem to have traded-off a significant number of deaths for the sake of little apparent benefit.
Ugh. Happened again!…
Maybe they will be able to “open up” more deeply and rapidly than other countries without there being spikes in infections – but again there isn’t evidence of that so far (they still have a much higher infection rate than other Nordic countries, which seem similarly “opened-up at this point).
A huge factorndoe evaluating their policies will be of there is a vaccine developed on a relatively short time horizon. If one is, then the per capita death rate in other Nordic countries will never reach the same level as Sweden – while the Swedish strategy is based on a theory that all countries will basically even out because the only thing that will stop the virus is reaching the herd immunity threshold because of the number of infections (as opposed to the influence of vaccinations).
As it is now, even if there are zero deaths going forward in Sweden even as they continue in other countries, it would take a country like Denmark or Norway or Taiwan or Korea or Finland or even Switzerland years if not decades to reach the same per capita death rate as Sweden if they continue with deaths at the rate they are currently experiencing.
I do think there are factors other than COVID deaths and the economy to consider, though. Mental health impacts, educational losses, and other negative effects of social disruption.
I think there are probably advantages to being closer to “normal life” that are not measured in either COVID deaths or immediate economic measures.
We won’t know how much of a difference this made for years, though.
Fair point. Although I would imagine that there are non-trivial mental health and social disruption “costs” differentially, from far greater # of deaths and serious illness.
Non-trivial, yes, but I think these costs are probably overestimated by most. 1957/1968 flu pandemics didn’t cause a lot of lasting trauma (family members who were around then don’t even remember they happened – but polio is remembered).
Infectious disease is less of an everyday reality now in the US & Western Europe due to vaccines, but still….
The huge differential in mortality risk by age probably reduces the expected social impact from COVID. That doesn’t make the deaths less tragic, especially if one of your family members, but it does make it less “shocking”/traumatic from a societal perspective.
confused –
> but I think these costs are probably overestimated by most.
Probably? I dunno. They could be underestimated. We don’t know the long term sequelae from this disease but there is some evidence they may be significant and long lasting. By definition the differences in sever illness across countries (roughly in line with infection rates) in absolute numbers will be much greater than the differences in deaths. Just off the bat things like lost productivity will be greater with greater illness. But given the potential for long-term sequelae…
Further, people are discovering more and more about the long term impact of trauma. Again I think that you are overly-confident in a particular directtion fairly uniformly. Not to say your sense of things is wrong – but that you may be too quick to find the scales of uncertainty tipping in a particular direction.
I don’t know how we determine what is and isn’t an “overestimation” let along characterize what some kind of global or generalizes “estimation” even is – but I think that rhe differential impact of increased severe illness and death are likely to be non-trivial.
>>By definition the differences in sever illness across countries (roughly in line with infection rates) in absolute numbers will be much greater than the differences in deaths. Just off the bat things like lost productivity will be greater with greater illness.
Sure. But the current disruptions to society will probably “swamp” any such effects – make them non-obvious.
I think something like 50% of working-age (say 18-65) people infected will be asymptomatic, and lots more will be mild enough to not be significantly impairing.
>>Further, people are discovering more and more about the long term impact of trauma.
Are you talking about physical harm from disease, or emotional trauma?
I am sure emotional trauma is important — but I think reactions to the disease have caused at least as much (probably more, outside places like NYC and Lombardy) emotional trauma as the actual disease.
I live in one of the states that looks worst right now (TX). None of the people I really *know* (co-workers, friends, or family) has had it (at least known they had it); and the 2 remote acquaintances (IE – people I’ve met like 5 years ago, but wouldn’t recognize on sight) I’ve heard had it weren’t particularly severe cases.
I think people understate how unique (at least in the “developed world” not sure about e.g. Sao Paulo or Mexico City) the Greater New York/Lombardy/etc. experience in March/April was.
>>Again I think that you are overly-confident in a particular directtion fairly uniformly. Not to say your sense of things is wrong – but that you may be too quick to find the scales of uncertainty tipping in a particular direction.
That’s quite possibly true!
I think this because to me historical examples of pandemics e.g. 1957, 1968, and even 1918 show that the social disruption is much less than would be expected from the numbers of deaths. The 1968 pandemic is barely remembered even though it is well within living memory.
So I have a fairly strong “prior” that a COVID pandemic that causes (say) 200,000 to 250,000 deaths in the US – 0.06 to 0.075% of the population – will have “direct social costs” – IE costs from illness and death, not from interventions to stop the spread – relatively comparable to the 1957-8 pandemic (~118,000 deaths – about 0.06% of the population of the time). IE – low enough that it is pretty much a historical footnote, barely mentioned.
But it is possible that current society really is *that* much more fragile.
I think any attempt at the *real* story of Sweden should make reference to these graphs:
https://www.gstatic.com/covid19/mobility/2020-07-14_SE_Mobility_Report_en.pdf
This is a google dataset on mobility changes relative to a normal year. Contrast Sweden with Norway:
https://www.gstatic.com/covid19/mobility/2020-07-14_NO_Mobility_Report_en.pdf
It may have taken longer to get going, but at least recently, on the population level, Sweden is actually more locked down than its scandanavian counterparts. The lesson of Sweden isn’t about whether it’s okay to open up, it’s that absent central direction, many people will adopt social distancing anyway. The fact that their stats look much worse than Norway then suggests that nevertheless, this sort of voluntary measure is less effective even for the same level of economic disruption, likely (IMO) due to individual superspreaders who do not voluntarily distance.
Zhao –
> The lesson of Sweden isn’t about whether it’s okay to open up, it’s that absent central direction, many people will adopt social distancing anyway.
I think that is likely influenced by culture/nationality I heard the joke in Sweden is that when they heard that social distancing would restrict people to remain six feet apart, a common reaction was “That close?”
Look at the differences in mask-wearing behavior in Korea or Japan vs. the US. Unlikely those differences are merely a result of official policy directives. Plus, in Sweden there are many societal factors that simply make it easier to isolate and social distance (smaller households, more jobs where you can work from home etc.)
Zhou, that is. Apologies.
I agree with that. A reopening US is not going to look like Sweden. In at least some ways, locked down US right now is more open than the supposedly open Sweden.
Well, the vast majority of the US isn’t locked down right now, in the sense of actual stay-at-home orders.
The big way in which life is more “normal” in Sweden was probably not closing many schools – but it is summer now.
The graphs are seasonally adjusted.
Oh, yes, I wasn’t really referring to the mobility data specifically. Just agreeing that much of the US right now (at least before school would start in a normal year) is not “more locked down” than Sweden.
The problem with the Sweden/Norway comparison is that most of Sweden’s deaths occurred early on – in April and early May. Many who died in April would have been infected in March, before any hypothetical lockdown would have occurred. We see Swedish mortality decrease as time goes on just as it did in most European countries (as well as some northern U.S. states).
It may be that Sweden’s fundamental problem was that the virus reached them sooner than their Nordic neighbors for whatever reason, during that critical March period. I am in Michigan, which similarly experienced early spread. Our state’s death curve actually looks remarkably similar to Sweden’s. We’ve recorded 6,366 Covid deaths as of today. Meanwhile, our neighbor to the south (Ohio) has recorded 3,189 deaths, despite having a larger population, and having adopted looser overall restrictions. For whatever reason, Michigan had more of the virus in March and that translated into a much worse April death toll.
Yeah, the recent drop in Swedish deaths looks pretty real by now, and is quite interesting.
Even if Sweden’s strategy turns out to be worse than others in Europe, considering all impacts, I think the effects seen in Sweden will be far less severe than would be predicted by most (non-Swedish) experts in March. Sweden will probably see a population fatality rate a bit worse than but roughly comparable to 1957/1968 pandemics… nothing like 1918.
*COVID deaths, COVID illness, changes in other illness/death due to response or resource-utilization impacts on care for other conditions, mental/social/emotional harm from the disease, avoided mental/emotional/social harm from stricter measures, economic effects, etc. etc.
I think Sweden has become so much a political issue it’s hard to discuss. I’m not even sure how their lockdown in practice differs that much from Finalnd and Norway, given that lots of people social distanced anyway (mobility was way down), and Sweden did close high schools and universities. The Finnish health authorities don’t believe that the decison to close schools in Finland had all that much an effect: they basically say it made no difference. Finland also closed restaurants/bars but not gyms or stores, but they did mandate no more than 10 people. That may have hjad more of an effect (especially bars). Sweden (or maybe Stockholm) has, I believe, a slightly higher percentage of people living alone (I believe it’s the highest in Europe), which probably also reduced the spread.
About judging it: it’s hard to know because the lockdown in the other Nordic countries was so short, so I’m not sure about whether Sweden will fare that much better in those other measures. First, there might be a sense in Norway and Finland that things are returning to normal whete Swedes don’t know when that will occur, and during that crucial March and April, the situation was so unclear that I suspect there wasn’t that much a difference in behaviour in the most of the people in the countries (but certianly in a smallish percentage of Swedes). So within the Noridc countries, the question could be whether a brief strict lockdown and then gradual reopening is better than letting it simmer indefinitely. It’s harder for places like the States, where lockdown just drags on and keeps getting lifted and then reintroduced. And maybe Sweden is better prepared for a second wave, although I’m hoping the numbers in the other Nordics are so small that they’ll be able to effectively trace and isolate.
Again, I don’t really know what in the long run will be determined to be the right decision. Ultimately, I think it’s going to as much a philosophical/ideological one, because there will be drawbacks and advantages of each approach, and people will differ on the tradeoffs.
Oh Sweden may very well turn out to be worse overall.
But I think it is nonetheless significant that the impacts seen were rather less than many would have predicted in March.
I now think it is very unlikely that any nation (at least of significant size say 10 million+) will see overall population death-rates of 0.2% or more (NYC was ~0.25%; highest nation now is San Marino at ~0.12%, but that is with 42 total deaths; the highest reasonably-sized nation is Belgium at about ~0.085%).
Predictions of 1.1 million deaths in US / 250,000 deaths in UK with “limited mitigation” (Sweden-like) (something like 0.33%-0.4% of population) over 12-18 months now look very unrealistic to me.
Given the current situation in the US, I don’t think we actually gained much by the measures taken in March/April… some benefit from delaying infections to allow treatment to be better understood, sure, but that’s maybe a factor of 2x at most I’d imagine. But I can’t really see the US winding up with 550,000 COVID deaths by early or mid-2021.
> the highest reasonably-sized nation is Belgium at about ~0.085%
Estimated death rates in Peru and Ecuador are 0.11% and 0.13%.
https://www.economist.com/graphic-detail/2020/07/15/tracking-covid-19-excess-deaths-across-countries
Yeah… I was simply drawing from the JHU source. I was not suggesting all nations *would* stop at ~0.085%. 0.2% maybe. But not 0.35%-0.7%.
I really wonder whether estimates based on excess deaths for these countries can be useful (usefully narrow error bars) at this point.
Also … some of these economies have way more people living on the edge of subsistence. I am not at all sure that excess deaths are a good proxy for COVID deaths (as they probably are in the US or Western Europe).
Maybe they are right. But then what % of Ecuador’s population would have to be infected by now??? Their median age is 28. Even with bad medical care their IFR would have to be pretty low…
Norway began introducing measures on the 12 March and Finland on the 16th. I believe that Norway and Sweden weren’t that far apart at the time: in all the Nordic countries, a lot of the initial covid infections were from people returning from ski holiday in Italy (roughly, these occur at much the same time in the three countries). So I don’t think the difference is that it reached Sweden earlier than Norway and not much earlier than in Finland.
The issue in Sweden may have been with problems in care facilities: even the Swedish authorities admit they messed up there. I guess one question could be whether the lockdowns in Norway and Finland reduced the spread within care facilities, because staff working in those centers and visitors (if there were even any in Finalnd and Norway) were less likely to be infected due to the lockdown. Of course, other measures than a lockdown could have prevented what happened in Swedish care centers as well. I’ve heard of lots of things that doesn’t make me surprised that fatalities were high in those facilities, and I imagine there will be lots of reports investigating the issue. But you could also argue that an initial lockdown would have bought them some time to figure out what was going on and take better steps,at protecting those in care facilities.
I think there is tons of uncertainty here.
In the US, there is South Dakota vs. Montana. Both very rural states.
South Dakota did little, and has seen a basically flat or very slowly declining rate of hospitalization for months.
Montana did more, hospitalizations dropped super low and are now rising.
So – if SD and MT are now both “open”, why are things getting worse in MT but not in SD?
Hospitalizations and deaths per million are still lower in MT than in SD — but SD doesn’t seem to have anywhere near enough for immunity to reduce R noticeably. SD is about 120 deaths. If we assume 0.5% IFR* that should mean about 24,000 infections — less than 3% of the population.
*lower than in Northeast or Italy/Spain, but I don’t think SD had big nursing home outbreaks, so it should be lower.
Some less-developed nations seem to be less affected than one would expect from the measures taken, as well.
Two weeks after my last comment on here, it really *does* look like the dramatic decline in deaths-per-day in Sweden is real.
Now, their total deaths are still in the top 10 worldwide, so that doesn’t mean it was a good strategy.
It does make it a lot harder to believe that the US ever could have seen >1 million deaths regardless of strategy, though. Sweden looks like it’s going to end up somewhere between 0.06%-0.07% of the total population. The US has more pre-existing conditions / worse preventive care, but on the other hand our median age is slightly lower. I can see the US doing somewhat worse, but not 5x worse.
You mean their per capita deaths.
Tegnell has said that many of their deaths in April were due to poor handling of nursing homes at the time, leading to outbreaks there. That isn’t necessarily related to them not shutting down their economy, considering that some countries that did shut down also witnessed outbreaks in nursing homes, too. Considering that this virus primarily preys on the elderly, that is a huge confounding factor.
But the fact that Sweden’s overall curve of deaths went steadily down, much like countries that locked down, suggests that the key variable isn’t closing your economy, it’s some other level of social distancing. (Because the Swedes *have* followed a number of social-distancing rules, they just haven’t forced businesses to close.)
Have you noticed thag (according to worldometers) Sweden is logging 5 deaths a day almost every day for the past several weeks? Why exactly 5? Seems fishy. Not your job to care, but thought I’d mention it.
Where do you see that? I see it fluctuating between zero and five.
https://www.worldometers.info/coronavirus/country/sweden/